Clay Sherrill, Jenna Port, Mohamad Wahoud, Ben Koethe, Sharanya Mohanty, Brian C Downey, Ayan Patel, Benjamin S Wessler
{"title":"超声心动图追踪主动脉瓣狭窄的进展。","authors":"Clay Sherrill, Jenna Port, Mohamad Wahoud, Ben Koethe, Sharanya Mohanty, Brian C Downey, Ayan Patel, Benjamin S Wessler","doi":"10.1186/s44156-025-00086-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transthoracic echocardiography (TTE) is used to assess aortic stenosis (AS) severity and track disease progression. As the field moves to study medical therapies to halt disease progression, reliable non-invasive imaging markers that are sensitive to small changes in disease progression are needed to enable efficient trial designs. The signal-to-noise ratio of commonly obtained TTE-based measures of progressive (non-severe) AS severity is unknown.</p><p><strong>Methods: </strong>This is a retrospective study of TTEs done at a tertiary referral centre (Tufts Medical Center, Boston MA). A cohort of patients with progressive AS who had two TTEs done within 30 days (in the absence of valve intervention) and a cohort of progressive AS patients with TTEs ≥ 1 year apart, also without valvular intervention, were assembled. Limits of agreement (LOA) and intraclass correlation (ICC) were calculated for aortic valve area (AVA) by continuity equation, peak velocity, and mean gradient. Cohen's d-statistic (d) was calculated for each hemodynamic assessment and a composite marker to assess sensitivity for detecting disease progression normalised to measurement variability.</p><p><strong>Results: </strong>The reproducibility cohort included 24 patients. The progression cohort included 35 patients. The median age was 70 years (interquartile range [IQR] 13). 22 patients (37.3%) were female. In the progression cohort, the median time between TTEs was 2.2 years (IQR 3.1 years). In the reproducibility cohort, AVA LOA were -0.7 to 0.8, ICC = 0.61; peak velocity LOA were -149.0 to + 126.7, ICC = 0.29; and mean gradient LOA were -16.2 to 12.2, ICC = 0.06. The d-statistic for annualised change in AVA was -0.29, the d-statistic for annualised change in maximum velocity was 0.46, the d-statistic for mean gradient was 0.55. The d-statistic for a composite, including all three hemodynamic markers, was 0.45.</p><p><strong>Conclusions: </strong>Standard TTE markers of AS severity have variable sensitivity for detecting AS progression. For patients with progressive (non-severe) AS, mean gradient has the highest signal-to-noise ratio and may be the most reliable TTE-based assessment of disease progression.</p>","PeriodicalId":45749,"journal":{"name":"Echo Research and Practice","volume":"12 1","pages":"19"},"PeriodicalIF":2.4000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12320324/pdf/","citationCount":"0","resultStr":"{\"title\":\"Tracking progression of aortic stenosis with echocardiography.\",\"authors\":\"Clay Sherrill, Jenna Port, Mohamad Wahoud, Ben Koethe, Sharanya Mohanty, Brian C Downey, Ayan Patel, Benjamin S Wessler\",\"doi\":\"10.1186/s44156-025-00086-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Transthoracic echocardiography (TTE) is used to assess aortic stenosis (AS) severity and track disease progression. As the field moves to study medical therapies to halt disease progression, reliable non-invasive imaging markers that are sensitive to small changes in disease progression are needed to enable efficient trial designs. The signal-to-noise ratio of commonly obtained TTE-based measures of progressive (non-severe) AS severity is unknown.</p><p><strong>Methods: </strong>This is a retrospective study of TTEs done at a tertiary referral centre (Tufts Medical Center, Boston MA). A cohort of patients with progressive AS who had two TTEs done within 30 days (in the absence of valve intervention) and a cohort of progressive AS patients with TTEs ≥ 1 year apart, also without valvular intervention, were assembled. Limits of agreement (LOA) and intraclass correlation (ICC) were calculated for aortic valve area (AVA) by continuity equation, peak velocity, and mean gradient. Cohen's d-statistic (d) was calculated for each hemodynamic assessment and a composite marker to assess sensitivity for detecting disease progression normalised to measurement variability.</p><p><strong>Results: </strong>The reproducibility cohort included 24 patients. The progression cohort included 35 patients. The median age was 70 years (interquartile range [IQR] 13). 22 patients (37.3%) were female. In the progression cohort, the median time between TTEs was 2.2 years (IQR 3.1 years). In the reproducibility cohort, AVA LOA were -0.7 to 0.8, ICC = 0.61; peak velocity LOA were -149.0 to + 126.7, ICC = 0.29; and mean gradient LOA were -16.2 to 12.2, ICC = 0.06. The d-statistic for annualised change in AVA was -0.29, the d-statistic for annualised change in maximum velocity was 0.46, the d-statistic for mean gradient was 0.55. The d-statistic for a composite, including all three hemodynamic markers, was 0.45.</p><p><strong>Conclusions: </strong>Standard TTE markers of AS severity have variable sensitivity for detecting AS progression. For patients with progressive (non-severe) AS, mean gradient has the highest signal-to-noise ratio and may be the most reliable TTE-based assessment of disease progression.</p>\",\"PeriodicalId\":45749,\"journal\":{\"name\":\"Echo Research and Practice\",\"volume\":\"12 1\",\"pages\":\"19\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-08-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12320324/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Echo Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44156-025-00086-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Echo Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44156-025-00086-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Tracking progression of aortic stenosis with echocardiography.
Background: Transthoracic echocardiography (TTE) is used to assess aortic stenosis (AS) severity and track disease progression. As the field moves to study medical therapies to halt disease progression, reliable non-invasive imaging markers that are sensitive to small changes in disease progression are needed to enable efficient trial designs. The signal-to-noise ratio of commonly obtained TTE-based measures of progressive (non-severe) AS severity is unknown.
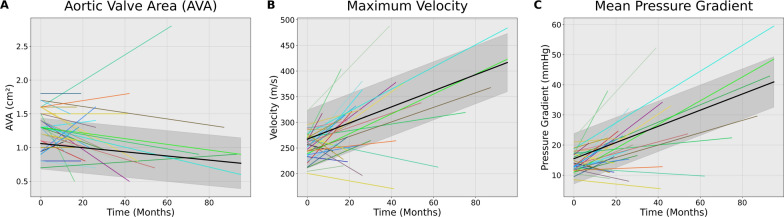
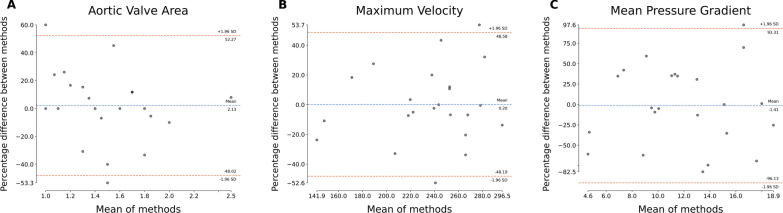
Methods: This is a retrospective study of TTEs done at a tertiary referral centre (Tufts Medical Center, Boston MA). A cohort of patients with progressive AS who had two TTEs done within 30 days (in the absence of valve intervention) and a cohort of progressive AS patients with TTEs ≥ 1 year apart, also without valvular intervention, were assembled. Limits of agreement (LOA) and intraclass correlation (ICC) were calculated for aortic valve area (AVA) by continuity equation, peak velocity, and mean gradient. Cohen's d-statistic (d) was calculated for each hemodynamic assessment and a composite marker to assess sensitivity for detecting disease progression normalised to measurement variability.
Results: The reproducibility cohort included 24 patients. The progression cohort included 35 patients. The median age was 70 years (interquartile range [IQR] 13). 22 patients (37.3%) were female. In the progression cohort, the median time between TTEs was 2.2 years (IQR 3.1 years). In the reproducibility cohort, AVA LOA were -0.7 to 0.8, ICC = 0.61; peak velocity LOA were -149.0 to + 126.7, ICC = 0.29; and mean gradient LOA were -16.2 to 12.2, ICC = 0.06. The d-statistic for annualised change in AVA was -0.29, the d-statistic for annualised change in maximum velocity was 0.46, the d-statistic for mean gradient was 0.55. The d-statistic for a composite, including all three hemodynamic markers, was 0.45.
Conclusions: Standard TTE markers of AS severity have variable sensitivity for detecting AS progression. For patients with progressive (non-severe) AS, mean gradient has the highest signal-to-noise ratio and may be the most reliable TTE-based assessment of disease progression.
期刊介绍:
Echo Research and Practice aims to be the premier international journal for physicians, sonographers, nurses and other allied health professionals practising echocardiography and other cardiac imaging modalities. This open-access journal publishes quality clinical and basic research, reviews, videos, education materials and selected high-interest case reports and videos across all echocardiography modalities and disciplines, including paediatrics, anaesthetics, general practice, acute medicine and intensive care. Multi-modality studies primarily featuring the use of cardiac ultrasound in clinical practice, in association with Cardiac Computed Tomography, Cardiovascular Magnetic Resonance or Nuclear Cardiology are of interest. Topics include, but are not limited to: 2D echocardiography 3D echocardiography Comparative imaging techniques – CCT, CMR and Nuclear Cardiology Congenital heart disease, including foetal echocardiography Contrast echocardiography Critical care echocardiography Deformation imaging Doppler echocardiography Interventional echocardiography Intracardiac echocardiography Intraoperative echocardiography Prosthetic valves Stress echocardiography Technical innovations Transoesophageal echocardiography Valve disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


