Rawad Halimeh, Joseph Klim, Lea Aoude, Marianne Bersaoui, Bernard Najib, Wiam Saab, Fadi Fakhoury, Rana Skaf
{"title":"妊娠33周严重免疫性血小板减少性紫癜1例报告。","authors":"Rawad Halimeh, Joseph Klim, Lea Aoude, Marianne Bersaoui, Bernard Najib, Wiam Saab, Fadi Fakhoury, Rana Skaf","doi":"10.18502/jri.v26i1.18782","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune thrombocytopenia (ITP) is an autoimmune condition that affects individuals of all ages, leading to a heightened risk of bleeding. ITP accounts for 5% of all pregnancy-related thrombocytopenia cases with an incidence of 1 in every 1,000 pregnant women. Several conditions can cause thrombocytopenia during pregnancy, making the diagnosis challenging. Current treatment of patients with ITP focuses on maintaining a safe platelet count rather than correcting it to normal levels.</p><p><strong>Case presentation: </strong>This article presents a case of a 26-year-old patient at 33 weeks of gestation with severe symptoms of thrombocytopenia, evidenced by a platelet count of 1000/<i>mm</i> <sup>3</sup>. The patient experienced self-resolving episodes of gingival bleeding, vaginal bleeding, and petechiae on her abdomen, as well as on both upper and lower extremities, over a duration of three days. She was successfully managed with prednisolone and intravenous immunoglobulin (IVIG), resulting in favorable maternal and neonatal outcomes.</p><p><strong>Conclusion: </strong>While there are currently no universally accepted guidelines for the treatment of ITP, expert consensus recommendations are available. Therefore, treatment should be individualized and closely monitored. A multidisciplinary team approach is essential for the effective management of ITP during pregnancy.</p>","PeriodicalId":38826,"journal":{"name":"Journal of Reproduction and Infertility","volume":"26 1","pages":"58-63"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317714/pdf/","citationCount":"0","resultStr":"{\"title\":\"Severe Immune Thrombocytopenic Purpura in a Patient at 33 Weeks of Gestation: A Case Report.\",\"authors\":\"Rawad Halimeh, Joseph Klim, Lea Aoude, Marianne Bersaoui, Bernard Najib, Wiam Saab, Fadi Fakhoury, Rana Skaf\",\"doi\":\"10.18502/jri.v26i1.18782\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Immune thrombocytopenia (ITP) is an autoimmune condition that affects individuals of all ages, leading to a heightened risk of bleeding. ITP accounts for 5% of all pregnancy-related thrombocytopenia cases with an incidence of 1 in every 1,000 pregnant women. Several conditions can cause thrombocytopenia during pregnancy, making the diagnosis challenging. Current treatment of patients with ITP focuses on maintaining a safe platelet count rather than correcting it to normal levels.</p><p><strong>Case presentation: </strong>This article presents a case of a 26-year-old patient at 33 weeks of gestation with severe symptoms of thrombocytopenia, evidenced by a platelet count of 1000/<i>mm</i> <sup>3</sup>. The patient experienced self-resolving episodes of gingival bleeding, vaginal bleeding, and petechiae on her abdomen, as well as on both upper and lower extremities, over a duration of three days. She was successfully managed with prednisolone and intravenous immunoglobulin (IVIG), resulting in favorable maternal and neonatal outcomes.</p><p><strong>Conclusion: </strong>While there are currently no universally accepted guidelines for the treatment of ITP, expert consensus recommendations are available. Therefore, treatment should be individualized and closely monitored. A multidisciplinary team approach is essential for the effective management of ITP during pregnancy.</p>\",\"PeriodicalId\":38826,\"journal\":{\"name\":\"Journal of Reproduction and Infertility\",\"volume\":\"26 1\",\"pages\":\"58-63\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317714/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Reproduction and Infertility\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18502/jri.v26i1.18782\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Reproduction and Infertility","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jri.v26i1.18782","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Severe Immune Thrombocytopenic Purpura in a Patient at 33 Weeks of Gestation: A Case Report.
Background: Immune thrombocytopenia (ITP) is an autoimmune condition that affects individuals of all ages, leading to a heightened risk of bleeding. ITP accounts for 5% of all pregnancy-related thrombocytopenia cases with an incidence of 1 in every 1,000 pregnant women. Several conditions can cause thrombocytopenia during pregnancy, making the diagnosis challenging. Current treatment of patients with ITP focuses on maintaining a safe platelet count rather than correcting it to normal levels.
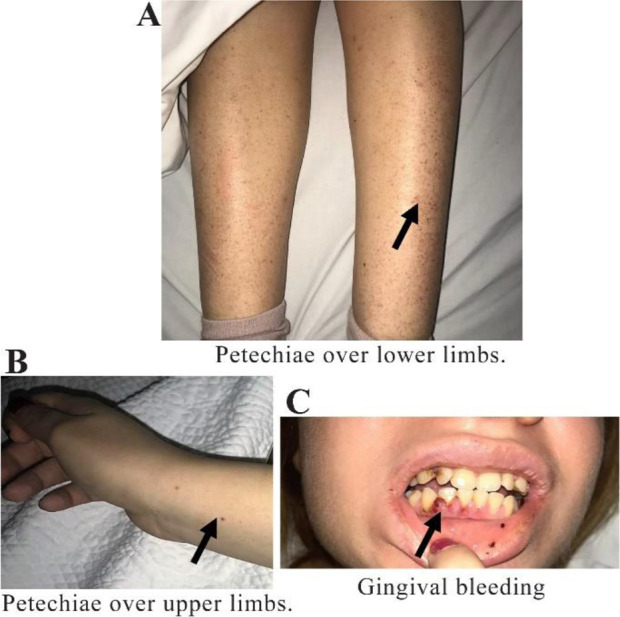
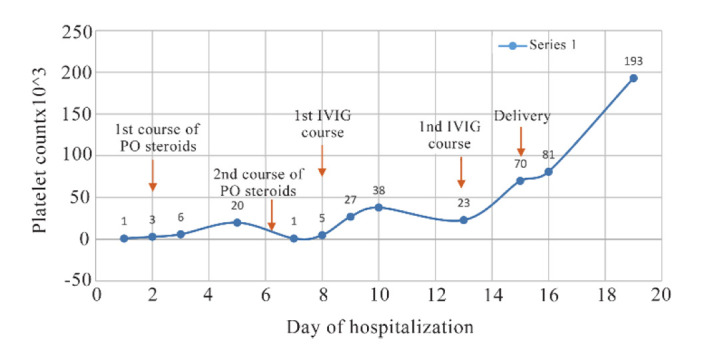
Case presentation: This article presents a case of a 26-year-old patient at 33 weeks of gestation with severe symptoms of thrombocytopenia, evidenced by a platelet count of 1000/mm3. The patient experienced self-resolving episodes of gingival bleeding, vaginal bleeding, and petechiae on her abdomen, as well as on both upper and lower extremities, over a duration of three days. She was successfully managed with prednisolone and intravenous immunoglobulin (IVIG), resulting in favorable maternal and neonatal outcomes.
Conclusion: While there are currently no universally accepted guidelines for the treatment of ITP, expert consensus recommendations are available. Therefore, treatment should be individualized and closely monitored. A multidisciplinary team approach is essential for the effective management of ITP during pregnancy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


