Jana L Anderson, Lucas Oliveira J E Silva, Erik P Hess, Derek E Vanmeter, Aidan Mullan, Juan P Brito, Ian G Hargraves, Fernanda Bellolio
{"title":"美国儿童急性中耳炎的共同决策:一项随机急诊科试验","authors":"Jana L Anderson, Lucas Oliveira J E Silva, Erik P Hess, Derek E Vanmeter, Aidan Mullan, Juan P Brito, Ian G Hargraves, Fernanda Bellolio","doi":"10.1186/s12873-025-01305-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Shared decision-making is increasingly utilized when multiple reasonable options exist. In the emergency department, however, several perceived barriers-such as time constraints, illness complexity, and varying levels of acceptance-limit its use. In cases of acute otitis media (AOM) in children, parental expectations for immediate antibiotic treatment often conflict with national guidelines recommending a trial of analgesics for 48 to 72 h prior to initiating antibiotics. As a result, antibiotic prescribing rates in the emergency department remain high, reaching up to 96%. Our aim was to measure the impact of the ear pain decision aid on parental knowledge, engagement and antibiotic use.</p><p><strong>Methods: </strong>We conducted a randomized trial in the Emergency Department and affiliated Urgent Care setting comparing shared decision-making with a web-based decision aid (earpaindecisionaid.org) to usual care for parents of children aged 6 months and older with non-severe AOM. Outcomes included parental knowledge of AOM, clinician/parent engagement, interaction time, and antibiotic use.</p><p><strong>Results: </strong>One hundred-one parents were enrolled; 42 participated in the Ear Pain Decision Aid (EPDA) arm using shared decision-making, while 59 received usual care (UC). Fifty-one interactions were videotaped. Parents in the EPDA arm scored greater in knowledge: EPDA 6.1 (1.74) vs. UC 5.1 (1.79), mean difference 1.0 (95% CI 0.3, 1.7), p = 0.004. They also scored high in decision-making: EPDA 14.7 (2.86) vs. UC 8.75 (3.68), mean difference 6.0 (95% CI 1.9, 10.0), p = 0.005. There was no significant difference in interaction time: EPDA 4.2 min (3.2, 5.6) vs. UC 3.0 min (2.4, 4.4), p = 0.059. No difference was detected in immediate antibiotic prescriptions: EPDA 36% vs. UC 42%, odds ratio 0.76 (95% CI 0.33, 1.71), p = 0.50. Similarly, no significant difference was found in wait-and-see prescription use: EPDA 64% vs. UC 6a8%, odds ratio 1.32 (95% CI 0.59, 2.99), p = 0.50.</p><p><strong>Conclusion: </strong>Shared decision-making with the Ear Pain Decision Aid (EPDA) improved parental knowledge and engagement without significantly increasing interaction time in the emergency department. Although no significant reduction in antibiotic prescribing was observed, this may be due to the study's limited sample size, which increases the risk of Type II error. These findings support the feasibility of integrating shared decision-making tools into emergency care. Larger, multicenter studies are needed to further evaluate the EPDA's effectiveness in promoting antibiotic stewardship for pediatric acute otitis media.</p><p><strong>Clinical trials number: </strong>NCT02872558 26/03/2017.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"146"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12318399/pdf/","citationCount":"0","resultStr":"{\"title\":\"Shared decision-making for pediatric acute otitis media in the United States: a randomized emergency department trial.\",\"authors\":\"Jana L Anderson, Lucas Oliveira J E Silva, Erik P Hess, Derek E Vanmeter, Aidan Mullan, Juan P Brito, Ian G Hargraves, Fernanda Bellolio\",\"doi\":\"10.1186/s12873-025-01305-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Shared decision-making is increasingly utilized when multiple reasonable options exist. In the emergency department, however, several perceived barriers-such as time constraints, illness complexity, and varying levels of acceptance-limit its use. In cases of acute otitis media (AOM) in children, parental expectations for immediate antibiotic treatment often conflict with national guidelines recommending a trial of analgesics for 48 to 72 h prior to initiating antibiotics. As a result, antibiotic prescribing rates in the emergency department remain high, reaching up to 96%. Our aim was to measure the impact of the ear pain decision aid on parental knowledge, engagement and antibiotic use.</p><p><strong>Methods: </strong>We conducted a randomized trial in the Emergency Department and affiliated Urgent Care setting comparing shared decision-making with a web-based decision aid (earpaindecisionaid.org) to usual care for parents of children aged 6 months and older with non-severe AOM. Outcomes included parental knowledge of AOM, clinician/parent engagement, interaction time, and antibiotic use.</p><p><strong>Results: </strong>One hundred-one parents were enrolled; 42 participated in the Ear Pain Decision Aid (EPDA) arm using shared decision-making, while 59 received usual care (UC). Fifty-one interactions were videotaped. Parents in the EPDA arm scored greater in knowledge: EPDA 6.1 (1.74) vs. UC 5.1 (1.79), mean difference 1.0 (95% CI 0.3, 1.7), p = 0.004. They also scored high in decision-making: EPDA 14.7 (2.86) vs. UC 8.75 (3.68), mean difference 6.0 (95% CI 1.9, 10.0), p = 0.005. There was no significant difference in interaction time: EPDA 4.2 min (3.2, 5.6) vs. UC 3.0 min (2.4, 4.4), p = 0.059. No difference was detected in immediate antibiotic prescriptions: EPDA 36% vs. UC 42%, odds ratio 0.76 (95% CI 0.33, 1.71), p = 0.50. Similarly, no significant difference was found in wait-and-see prescription use: EPDA 64% vs. UC 6a8%, odds ratio 1.32 (95% CI 0.59, 2.99), p = 0.50.</p><p><strong>Conclusion: </strong>Shared decision-making with the Ear Pain Decision Aid (EPDA) improved parental knowledge and engagement without significantly increasing interaction time in the emergency department. Although no significant reduction in antibiotic prescribing was observed, this may be due to the study's limited sample size, which increases the risk of Type II error. These findings support the feasibility of integrating shared decision-making tools into emergency care. Larger, multicenter studies are needed to further evaluate the EPDA's effectiveness in promoting antibiotic stewardship for pediatric acute otitis media.</p><p><strong>Clinical trials number: </strong>NCT02872558 26/03/2017.</p>\",\"PeriodicalId\":9002,\"journal\":{\"name\":\"BMC Emergency Medicine\",\"volume\":\"25 1\",\"pages\":\"146\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12318399/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12873-025-01305-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01305-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:当存在多种合理的选择时,共享决策的使用越来越多。然而,在急诊科,一些可感知的障碍——如时间限制、疾病复杂性和不同程度的接受程度——限制了它的使用。在儿童急性中耳炎(AOM)的病例中,父母对立即使用抗生素治疗的期望往往与国家指南建议在开始使用抗生素之前进行48至72小时的止痛药试验相冲突。因此,急诊科的抗生素处方率仍然很高,高达96%。我们的目的是衡量耳痛决策辅助对父母知识、参与和抗生素使用的影响。方法:我们在急诊科和附属紧急护理机构进行了一项随机试验,比较基于网络的决策辅助(earpaindecisionaid.org)与常规护理对6个月及以上非严重急性中耳炎儿童父母的共同决策。结果包括家长对AOM的了解、临床医生/家长参与、互动时间和抗生素使用。结果:共纳入家长101名;42名患者参与了耳痛决策辅助(EPDA)组,采用共同决策,59名患者接受常规护理(UC)。51次互动被录了下来。EPDA组的父母在知识方面得分更高:EPDA为6.1 (1.74),UC为5.1(1.79),平均差异为1.0 (95% CI 0.3, 1.7), p = 0.004。他们在决策方面也得分很高:EPDA为14.7 (2.86),UC为8.75(3.68),平均差异为6.0 (95% CI 1.9, 10.0), p = 0.005。相互作用时间差异无统计学意义:EPDA 4.2 min(3.2, 5.6)与UC 3.0 min (2.4, 4.4), p = 0.059。即时抗生素处方中未发现差异:EPDA 36% vs UC 42%,优势比0.76 (95% CI 0.33, 1.71), p = 0.50。同样,在等待和观察处方使用方面没有发现显著差异:EPDA 64% vs UC 6a8%,优势比1.32 (95% CI 0.59, 2.99), p = 0.50。结论:耳部疼痛辅助决策(EPDA)的共同决策提高了家长的知识和参与,但没有显著增加急诊互动时间。虽然没有观察到抗生素处方显著减少,但这可能是由于研究样本量有限,这增加了II型错误的风险。这些发现支持将共享决策工具整合到急诊护理中的可行性。需要更大的、多中心的研究来进一步评估EPDA在促进儿科急性中耳炎抗生素管理方面的有效性。临床试验编号:NCT02872558 26/03/2017。
Shared decision-making for pediatric acute otitis media in the United States: a randomized emergency department trial.
Background: Shared decision-making is increasingly utilized when multiple reasonable options exist. In the emergency department, however, several perceived barriers-such as time constraints, illness complexity, and varying levels of acceptance-limit its use. In cases of acute otitis media (AOM) in children, parental expectations for immediate antibiotic treatment often conflict with national guidelines recommending a trial of analgesics for 48 to 72 h prior to initiating antibiotics. As a result, antibiotic prescribing rates in the emergency department remain high, reaching up to 96%. Our aim was to measure the impact of the ear pain decision aid on parental knowledge, engagement and antibiotic use.
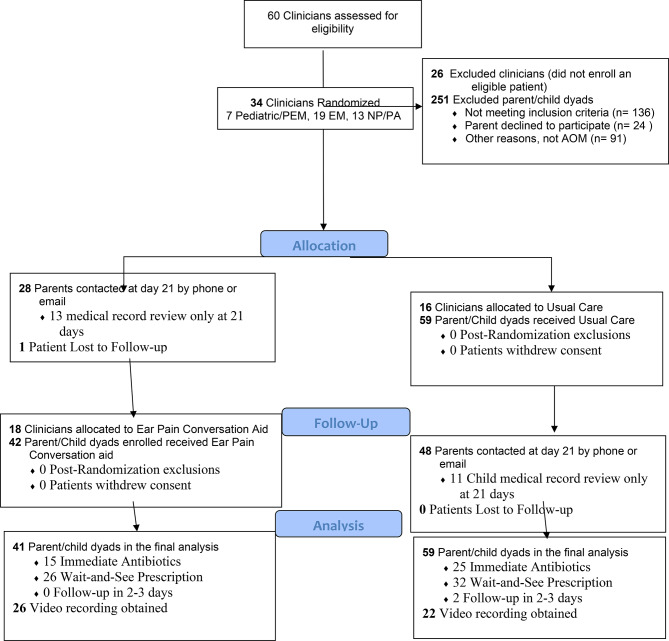
Methods: We conducted a randomized trial in the Emergency Department and affiliated Urgent Care setting comparing shared decision-making with a web-based decision aid (earpaindecisionaid.org) to usual care for parents of children aged 6 months and older with non-severe AOM. Outcomes included parental knowledge of AOM, clinician/parent engagement, interaction time, and antibiotic use.
Results: One hundred-one parents were enrolled; 42 participated in the Ear Pain Decision Aid (EPDA) arm using shared decision-making, while 59 received usual care (UC). Fifty-one interactions were videotaped. Parents in the EPDA arm scored greater in knowledge: EPDA 6.1 (1.74) vs. UC 5.1 (1.79), mean difference 1.0 (95% CI 0.3, 1.7), p = 0.004. They also scored high in decision-making: EPDA 14.7 (2.86) vs. UC 8.75 (3.68), mean difference 6.0 (95% CI 1.9, 10.0), p = 0.005. There was no significant difference in interaction time: EPDA 4.2 min (3.2, 5.6) vs. UC 3.0 min (2.4, 4.4), p = 0.059. No difference was detected in immediate antibiotic prescriptions: EPDA 36% vs. UC 42%, odds ratio 0.76 (95% CI 0.33, 1.71), p = 0.50. Similarly, no significant difference was found in wait-and-see prescription use: EPDA 64% vs. UC 6a8%, odds ratio 1.32 (95% CI 0.59, 2.99), p = 0.50.
Conclusion: Shared decision-making with the Ear Pain Decision Aid (EPDA) improved parental knowledge and engagement without significantly increasing interaction time in the emergency department. Although no significant reduction in antibiotic prescribing was observed, this may be due to the study's limited sample size, which increases the risk of Type II error. These findings support the feasibility of integrating shared decision-making tools into emergency care. Larger, multicenter studies are needed to further evaluate the EPDA's effectiveness in promoting antibiotic stewardship for pediatric acute otitis media.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


