{"title":"生命体征在预测急诊科老年患者死亡风险中的作用。","authors":"Karin Erwander, Björn Agvall, Kjell Ivarsson","doi":"10.1186/s12873-025-01307-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Accurate risk stratification in older adults presenting to the emergency department (ED) is essential but challenging due to atypical presentations and age-related physiological changes. While vital signs are central to triage, their predictive value for short-term mortality in this population remains unclear. This study aimed to explore the association between initial vital signs and 7-day mortality among older ED patients.</p><p><strong>Method: </strong>This retrospective cohort study included patients aged ≥ 65 years who visited two EDs in Region Halland, Sweden, during 2018. Vital signs, systolic blood pressure (SBP), heart rate (HR), peripheral oxygen saturation (SpO₂), respiratory rate (RR), body temperature, and level of consciousness (LOC), were extracted from the regional health information system. Descriptive statistics, ROC curve analysis, and logistic regression were used to assess associations between categorized vital signs and 7-day mortality, adjusting for age, sex, and comorbidity.</p><p><strong>Results: </strong>Of 30 327 ED visits, 25 450 patients had at least one recorded vital sign. The mean age was 78 years; 50% were female. The 7-day mortality rate was 2%. ROC analysis showed limited discriminative ability of individual vital signs (AUC range: 0.49-0.70). Low SBP, high HR, low SpO₂, and impaired LOC were statistically significantly associated with mortality. Multivariable logistic regression confirmed these associations, with SBP (≤ 80 mmHg, AOR 7.79; 95% CI 3.27-18.54), high HR (> 125 bpm, AOR 6.37; 95% CI 1.26-32.16), low SpO₂ (≤ 80%, AOR 3.64; 95% CI 1.75-7.58), and impaired LOC (GCS < 13 (AOR 9.30-18.36)) showing the strongest effects.</p><p><strong>Conclusion: </strong>Low SBP, elevated HR, reduced SpO₂, and impaired LOC were independently associated with short-term mortality in older ED patients, though their individual predictive performance was modest. LOC, despite being a strong predictor, was frequently missing, underscoring challenges in routine assessment. These findings highlight the need for more comprehensive, geriatric-informed triage systems that incorporate age-related physiological changes and ensure consistent evaluation of LOC. As frailty and functional status was not available in this dataset, future studies should focus on integrated models that include these factors to improve early risk identification in emergency care for older adults.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"144"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317628/pdf/","citationCount":"0","resultStr":"{\"title\":\"The role of vital signs in predicting mortality risk in elderly patients visiting the emergency department.\",\"authors\":\"Karin Erwander, Björn Agvall, Kjell Ivarsson\",\"doi\":\"10.1186/s12873-025-01307-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Accurate risk stratification in older adults presenting to the emergency department (ED) is essential but challenging due to atypical presentations and age-related physiological changes. While vital signs are central to triage, their predictive value for short-term mortality in this population remains unclear. This study aimed to explore the association between initial vital signs and 7-day mortality among older ED patients.</p><p><strong>Method: </strong>This retrospective cohort study included patients aged ≥ 65 years who visited two EDs in Region Halland, Sweden, during 2018. Vital signs, systolic blood pressure (SBP), heart rate (HR), peripheral oxygen saturation (SpO₂), respiratory rate (RR), body temperature, and level of consciousness (LOC), were extracted from the regional health information system. Descriptive statistics, ROC curve analysis, and logistic regression were used to assess associations between categorized vital signs and 7-day mortality, adjusting for age, sex, and comorbidity.</p><p><strong>Results: </strong>Of 30 327 ED visits, 25 450 patients had at least one recorded vital sign. The mean age was 78 years; 50% were female. The 7-day mortality rate was 2%. ROC analysis showed limited discriminative ability of individual vital signs (AUC range: 0.49-0.70). Low SBP, high HR, low SpO₂, and impaired LOC were statistically significantly associated with mortality. Multivariable logistic regression confirmed these associations, with SBP (≤ 80 mmHg, AOR 7.79; 95% CI 3.27-18.54), high HR (> 125 bpm, AOR 6.37; 95% CI 1.26-32.16), low SpO₂ (≤ 80%, AOR 3.64; 95% CI 1.75-7.58), and impaired LOC (GCS < 13 (AOR 9.30-18.36)) showing the strongest effects.</p><p><strong>Conclusion: </strong>Low SBP, elevated HR, reduced SpO₂, and impaired LOC were independently associated with short-term mortality in older ED patients, though their individual predictive performance was modest. LOC, despite being a strong predictor, was frequently missing, underscoring challenges in routine assessment. These findings highlight the need for more comprehensive, geriatric-informed triage systems that incorporate age-related physiological changes and ensure consistent evaluation of LOC. As frailty and functional status was not available in this dataset, future studies should focus on integrated models that include these factors to improve early risk identification in emergency care for older adults.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>\",\"PeriodicalId\":9002,\"journal\":{\"name\":\"BMC Emergency Medicine\",\"volume\":\"25 1\",\"pages\":\"144\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12317628/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12873-025-01307-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01307-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:在急诊科(ED)的老年人中,准确的风险分层是必要的,但由于不典型的表现和与年龄相关的生理变化,这是具有挑战性的。虽然生命体征是分诊的核心,但它们对这一人群短期死亡率的预测价值仍不清楚。本研究旨在探讨老年ED患者初始生命体征与7天死亡率之间的关系。方法:本回顾性队列研究纳入了2018年在瑞典哈兰地区就诊的两家急诊科年龄≥65岁的患者。生命体征、收缩压(SBP)、心率(HR)、外周血氧饱和度(SpO₂)、呼吸频率(RR)、体温和意识水平(LOC)从区域卫生信息系统中提取。采用描述性统计、ROC曲线分析和逻辑回归来评估分类生命体征与7天死亡率之间的关系,并对年龄、性别和合并症进行校正。结果:在30327例急诊科就诊中,25450例患者至少有一个生命体征记录。平均年龄78岁;50%是女性。7天死亡率为2%。ROC分析显示个体生命体征的判别能力有限(AUC范围:0.49 ~ 0.70)。低收缩压、高HR、低spo2和LOC受损与死亡率有统计学显著相关。多变量logistic回归证实了这些相关性,收缩压(≤80 mmHg, AOR 7.79;95% CI 3.27-18.54),高HR (> 125 bpm, AOR 6.37;95% CI 1.26-32.16),低SpO₂(≤80%,AOR 3.64;结论:低收缩压、HR升高、SpO₂减少和LOC受损与老年ED患者的短期死亡率独立相关,尽管它们的个体预测性能不高。尽管LOC是一个强有力的预测指标,但它经常被遗漏,这凸显了常规评估中的挑战。这些发现强调需要更全面的老年医学分类系统,包括与年龄相关的生理变化,并确保对LOC的一致评估。由于该数据集中没有虚弱和功能状态,未来的研究应侧重于包括这些因素的综合模型,以提高老年人急诊护理的早期风险识别。临床试验号:不适用。
The role of vital signs in predicting mortality risk in elderly patients visiting the emergency department.
Background: Accurate risk stratification in older adults presenting to the emergency department (ED) is essential but challenging due to atypical presentations and age-related physiological changes. While vital signs are central to triage, their predictive value for short-term mortality in this population remains unclear. This study aimed to explore the association between initial vital signs and 7-day mortality among older ED patients.
Method: This retrospective cohort study included patients aged ≥ 65 years who visited two EDs in Region Halland, Sweden, during 2018. Vital signs, systolic blood pressure (SBP), heart rate (HR), peripheral oxygen saturation (SpO₂), respiratory rate (RR), body temperature, and level of consciousness (LOC), were extracted from the regional health information system. Descriptive statistics, ROC curve analysis, and logistic regression were used to assess associations between categorized vital signs and 7-day mortality, adjusting for age, sex, and comorbidity.
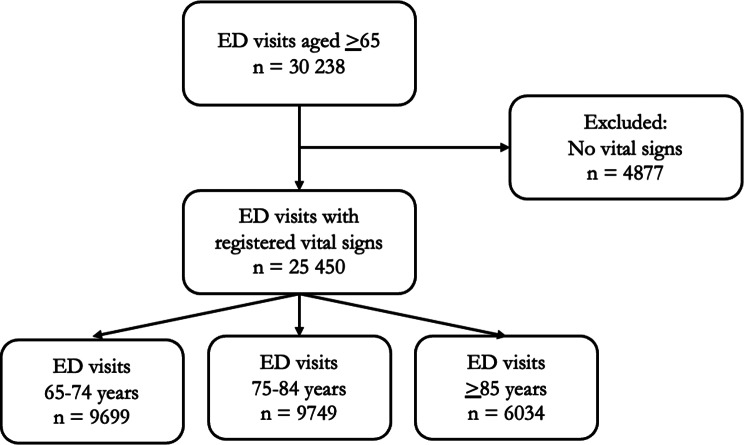
Results: Of 30 327 ED visits, 25 450 patients had at least one recorded vital sign. The mean age was 78 years; 50% were female. The 7-day mortality rate was 2%. ROC analysis showed limited discriminative ability of individual vital signs (AUC range: 0.49-0.70). Low SBP, high HR, low SpO₂, and impaired LOC were statistically significantly associated with mortality. Multivariable logistic regression confirmed these associations, with SBP (≤ 80 mmHg, AOR 7.79; 95% CI 3.27-18.54), high HR (> 125 bpm, AOR 6.37; 95% CI 1.26-32.16), low SpO₂ (≤ 80%, AOR 3.64; 95% CI 1.75-7.58), and impaired LOC (GCS < 13 (AOR 9.30-18.36)) showing the strongest effects.
Conclusion: Low SBP, elevated HR, reduced SpO₂, and impaired LOC were independently associated with short-term mortality in older ED patients, though their individual predictive performance was modest. LOC, despite being a strong predictor, was frequently missing, underscoring challenges in routine assessment. These findings highlight the need for more comprehensive, geriatric-informed triage systems that incorporate age-related physiological changes and ensure consistent evaluation of LOC. As frailty and functional status was not available in this dataset, future studies should focus on integrated models that include these factors to improve early risk identification in emergency care for older adults.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


