Francesca Graziano, Elena Cozza, Antonella Millin, Alessandro Gianni, Giulia Mattesi, Raffaella Motta, Francesco Peruzza, Alessio Micchi, Carmelo Cicciò, Francesco Zamboni, Domenico Corrado, Roberto Filippini, Valeria Pergola, Alessandro Zorzi
{"title":"运动前试验中st段下降或高危室性早搏的运动健将冠脉疾病的患病率及特点","authors":"Francesca Graziano, Elena Cozza, Antonella Millin, Alessandro Gianni, Giulia Mattesi, Raffaella Motta, Francesco Peruzza, Alessio Micchi, Carmelo Cicciò, Francesco Zamboni, Domenico Corrado, Roberto Filippini, Valeria Pergola, Alessandro Zorzi","doi":"10.1093/ehjopen/oeaf090","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Whether exercise stress testing (ET) for early identification of coronary artery disease (CAD) should be performed for preparticipation screening (PPS) in all master athletes (MAs) or in high-risk athletes only remains debated. We evaluated the prevalence and characteristics of CAD in MAs who underwent coronary computed tomography angiography (CCTA) after a positive preparticipation ET.</p><p><strong>Methods and results: </strong>According to Italian law and guidelines, all MAs ≥40 years old must undergo annual ET as part of PPS. We retrospectively enrolled MAs without symptoms, baseline ECG abnormalities or history of heart disease referred to CCTA for ST-segment depression (STD) and/or high-risk premature ventricular beats (PVBs) during ET. We evaluated CAD burden, plaque characteristics, and pericoronary fat attenuation index. Athletes with at-risk PVBs also underwent cardiac magnetic resonance (CMR). We enrolled 130 Caucasian MAs (84% males, median age 54 years): 49 (37%) with high-risk PVBs, and 82 (62%) with STD. Coronary artery disease with ≥50% stenosis was identified in 17 (13%) MAs, including 1 with high-risk plaques, without differences according to CCTA indications (<i>P</i> = 0.83). Age ≥ 60 years and dyslipidemia were independent predictors of ≥50% stenosis, and none of the 45 athletes without risk factors had CAD. Only three athletes eventually required coronary revascularization. Among MAs with PVBs, 20/49 (41%) had abnormal CMR and one cathecolaminergic polymorphic ventricular tachycardia.</p><p><strong>Conclusion: </strong>In a sample of asymptomatic MAs, STD and PVBs during ET were poor predictors for the presence of significant CAD, strongly influenced by the presence of traditional cardiovascular risk factors. However, ET may have a broader diagnostic value by identifying exercise-induced PVBs, enabling the detection of concealed arrhythmogenic conditions.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 4","pages":"oeaf090"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12311791/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prevalence and characteristics of coronary artery disease in master athletes with ST-segment depression or high-risk premature ventricular beats at pre-participation exercise testing.\",\"authors\":\"Francesca Graziano, Elena Cozza, Antonella Millin, Alessandro Gianni, Giulia Mattesi, Raffaella Motta, Francesco Peruzza, Alessio Micchi, Carmelo Cicciò, Francesco Zamboni, Domenico Corrado, Roberto Filippini, Valeria Pergola, Alessandro Zorzi\",\"doi\":\"10.1093/ehjopen/oeaf090\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Whether exercise stress testing (ET) for early identification of coronary artery disease (CAD) should be performed for preparticipation screening (PPS) in all master athletes (MAs) or in high-risk athletes only remains debated. We evaluated the prevalence and characteristics of CAD in MAs who underwent coronary computed tomography angiography (CCTA) after a positive preparticipation ET.</p><p><strong>Methods and results: </strong>According to Italian law and guidelines, all MAs ≥40 years old must undergo annual ET as part of PPS. We retrospectively enrolled MAs without symptoms, baseline ECG abnormalities or history of heart disease referred to CCTA for ST-segment depression (STD) and/or high-risk premature ventricular beats (PVBs) during ET. We evaluated CAD burden, plaque characteristics, and pericoronary fat attenuation index. Athletes with at-risk PVBs also underwent cardiac magnetic resonance (CMR). We enrolled 130 Caucasian MAs (84% males, median age 54 years): 49 (37%) with high-risk PVBs, and 82 (62%) with STD. Coronary artery disease with ≥50% stenosis was identified in 17 (13%) MAs, including 1 with high-risk plaques, without differences according to CCTA indications (<i>P</i> = 0.83). Age ≥ 60 years and dyslipidemia were independent predictors of ≥50% stenosis, and none of the 45 athletes without risk factors had CAD. Only three athletes eventually required coronary revascularization. Among MAs with PVBs, 20/49 (41%) had abnormal CMR and one cathecolaminergic polymorphic ventricular tachycardia.</p><p><strong>Conclusion: </strong>In a sample of asymptomatic MAs, STD and PVBs during ET were poor predictors for the presence of significant CAD, strongly influenced by the presence of traditional cardiovascular risk factors. However, ET may have a broader diagnostic value by identifying exercise-induced PVBs, enabling the detection of concealed arrhythmogenic conditions.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 4\",\"pages\":\"oeaf090\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12311791/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf090\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf090","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Prevalence and characteristics of coronary artery disease in master athletes with ST-segment depression or high-risk premature ventricular beats at pre-participation exercise testing.
Aims: Whether exercise stress testing (ET) for early identification of coronary artery disease (CAD) should be performed for preparticipation screening (PPS) in all master athletes (MAs) or in high-risk athletes only remains debated. We evaluated the prevalence and characteristics of CAD in MAs who underwent coronary computed tomography angiography (CCTA) after a positive preparticipation ET.
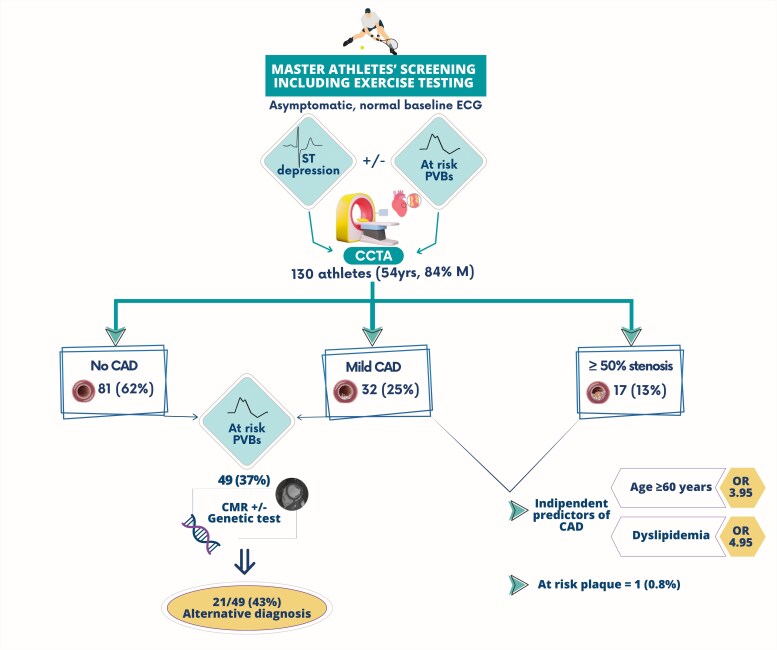
Methods and results: According to Italian law and guidelines, all MAs ≥40 years old must undergo annual ET as part of PPS. We retrospectively enrolled MAs without symptoms, baseline ECG abnormalities or history of heart disease referred to CCTA for ST-segment depression (STD) and/or high-risk premature ventricular beats (PVBs) during ET. We evaluated CAD burden, plaque characteristics, and pericoronary fat attenuation index. Athletes with at-risk PVBs also underwent cardiac magnetic resonance (CMR). We enrolled 130 Caucasian MAs (84% males, median age 54 years): 49 (37%) with high-risk PVBs, and 82 (62%) with STD. Coronary artery disease with ≥50% stenosis was identified in 17 (13%) MAs, including 1 with high-risk plaques, without differences according to CCTA indications (P = 0.83). Age ≥ 60 years and dyslipidemia were independent predictors of ≥50% stenosis, and none of the 45 athletes without risk factors had CAD. Only three athletes eventually required coronary revascularization. Among MAs with PVBs, 20/49 (41%) had abnormal CMR and one cathecolaminergic polymorphic ventricular tachycardia.
Conclusion: In a sample of asymptomatic MAs, STD and PVBs during ET were poor predictors for the presence of significant CAD, strongly influenced by the presence of traditional cardiovascular risk factors. However, ET may have a broader diagnostic value by identifying exercise-induced PVBs, enabling the detection of concealed arrhythmogenic conditions.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


