Christopher Remmington, Luigi Camporota, Daniel Taylor, Angelo Sousa, Barnaby Sanderson, Guy Glover
{"title":"近致死性哮喘患者接受挥发性麻醉药治疗的特点和结果:一项回顾性观察队列研究。","authors":"Christopher Remmington, Luigi Camporota, Daniel Taylor, Angelo Sousa, Barnaby Sanderson, Guy Glover","doi":"10.1097/CCE.0000000000001295","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance and objectives: </strong>Inhaled volatile anesthetics are employed as rescue therapy in near-fatal asthma, despite limited evidence. This study aims to describe the characteristics, management, and outcomes of mechanically ventilated adult patients with near-fatal asthma, stratified by the use of volatile anesthetic therapy.</p><p><strong>Design: </strong>Retrospective single-center observational cohort study.</p><p><strong>Setting: </strong>Tertiary critical care and extracorporeal membrane oxygenation (ECMO) unit.</p><p><strong>Participants: </strong>Adults 16 years old or older receiving mechanical ventilation (MV) for greater than or equal to 24 hours and/or ECMO between January 2016 and August 2023 for near-fatal asthma.</p><p><strong>Main outcomes and measures: </strong>We recorded demographics, disease severity tidal volumes, and ventilator settings, by treatment over the first 100 hours. Outcomes were duration of ECMO and MV, ICU length of stay, 90-day mortality, and adverse drug reaction.</p><p><strong>Results: </strong>Sixty-two patients were included (62.9% female), with a median (interquartile range [IQR]) age of 45 years (29-51 yr). Median (IQR) pH 7.13 (6.93-7.23), Paco2 12.9 kPa (8.7-16.2 kPa), and tidal volume 178 mL (50-300 mL). Most patients received IV bronchodilators and 32 (51.6%) required ECMO. Thirty-eight patients (61.3%) were treated with volatile anesthetics. Volatile patients had worse ventilation and blood gas parameters before treatment, more barotrauma, and were more likely to be receiving ECMO. Despite this, improvements in tidal volume occurred in the volatile group (mean increase, 204 mL [83.9%]; 95% CI, 110-298; p < 0.001). Median (IQR) duration of MV and ICU length of stay in volatile and no volatile patients were 10 days (8-16 d) vs. 5 days (3-10 d; p = 0.001) and 15 days (13-20 d) vs. 9 days (7-14 d; p = 0.001), respectively. ICU and 90-day mortality in volatile and no volatile patients were 5.3% vs. 4.2%.</p><p><strong>Conclusions and relevance: </strong>The use of inhaled volatile anesthetics for near-fatal asthma, including during ECMO, appears to be feasible and safe, and with favorable clinical outcomes; however, no conclusions regarding efficacy can be directly inferred.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 8","pages":"e1295"},"PeriodicalIF":2.7000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12316345/pdf/","citationCount":"0","resultStr":"{\"title\":\"Characteristics and Outcomes of Patients Receiving Volatile Anesthetics in Near-Fatal Asthma: A Retrospective Observational Cohort Study.\",\"authors\":\"Christopher Remmington, Luigi Camporota, Daniel Taylor, Angelo Sousa, Barnaby Sanderson, Guy Glover\",\"doi\":\"10.1097/CCE.0000000000001295\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance and objectives: </strong>Inhaled volatile anesthetics are employed as rescue therapy in near-fatal asthma, despite limited evidence. This study aims to describe the characteristics, management, and outcomes of mechanically ventilated adult patients with near-fatal asthma, stratified by the use of volatile anesthetic therapy.</p><p><strong>Design: </strong>Retrospective single-center observational cohort study.</p><p><strong>Setting: </strong>Tertiary critical care and extracorporeal membrane oxygenation (ECMO) unit.</p><p><strong>Participants: </strong>Adults 16 years old or older receiving mechanical ventilation (MV) for greater than or equal to 24 hours and/or ECMO between January 2016 and August 2023 for near-fatal asthma.</p><p><strong>Main outcomes and measures: </strong>We recorded demographics, disease severity tidal volumes, and ventilator settings, by treatment over the first 100 hours. Outcomes were duration of ECMO and MV, ICU length of stay, 90-day mortality, and adverse drug reaction.</p><p><strong>Results: </strong>Sixty-two patients were included (62.9% female), with a median (interquartile range [IQR]) age of 45 years (29-51 yr). Median (IQR) pH 7.13 (6.93-7.23), Paco2 12.9 kPa (8.7-16.2 kPa), and tidal volume 178 mL (50-300 mL). Most patients received IV bronchodilators and 32 (51.6%) required ECMO. Thirty-eight patients (61.3%) were treated with volatile anesthetics. Volatile patients had worse ventilation and blood gas parameters before treatment, more barotrauma, and were more likely to be receiving ECMO. Despite this, improvements in tidal volume occurred in the volatile group (mean increase, 204 mL [83.9%]; 95% CI, 110-298; p < 0.001). Median (IQR) duration of MV and ICU length of stay in volatile and no volatile patients were 10 days (8-16 d) vs. 5 days (3-10 d; p = 0.001) and 15 days (13-20 d) vs. 9 days (7-14 d; p = 0.001), respectively. ICU and 90-day mortality in volatile and no volatile patients were 5.3% vs. 4.2%.</p><p><strong>Conclusions and relevance: </strong>The use of inhaled volatile anesthetics for near-fatal asthma, including during ECMO, appears to be feasible and safe, and with favorable clinical outcomes; however, no conclusions regarding efficacy can be directly inferred.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 8\",\"pages\":\"e1295\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-07-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12316345/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001295\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001295","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
重要性和目的:尽管证据有限,但吸入挥发性麻醉药仍被用作近致死性哮喘的抢救治疗。本研究旨在描述机械通气的成人哮喘患者的特征、管理和结果,并通过使用挥发性麻醉治疗进行分层。设计:回顾性单中心观察队列研究。环境:三级重症监护和体外膜氧合(ECMO)单位。参与者:2016年1月至2023年8月期间接受机械通气(MV)大于或等于24小时和/或ECMO的16岁或以上成年人,用于治疗接近致命性的哮喘。主要结局和指标:通过前100小时的治疗,我们记录了人口统计学、疾病严重程度、潮汐量和呼吸机设置。结果为ECMO和MV持续时间、ICU住院时间、90天死亡率和药物不良反应。结果:纳入62例患者(62.9%为女性),中位年龄(四分位数间距[IQR])为45岁(29-51岁)。中位数(IQR) pH为7.13 (6.93-7.23),Paco2为12.9 kPa (8.7-16.2 kPa),潮气量为178 mL (50-300 mL)。大多数患者接受静脉支气管扩张剂治疗,32例(51.6%)患者需要ECMO。38例(61.3%)患者使用了挥发性麻醉剂。易挥发患者在治疗前通气和血气参数较差,气压损伤较多,更有可能接受ECMO。尽管如此,挥发油组的潮气量有所改善(平均增加204 mL [83.9%];95% ci, 110-298;P < 0.001)。挥发性和非挥发性患者的中位数(IQR) MV持续时间和ICU住院时间分别为10天(8-16天)和5天(3-10天);P = 0.001)和15天(13-20 d) vs. 9天(7-14 d;P = 0.001)。反复发作和无反复发作患者的ICU和90天死亡率分别为5.3%和4.2%。结论和相关性:吸入挥发性麻醉药用于近致死性哮喘,包括在ECMO期间,似乎是可行和安全的,并且具有良好的临床结果;然而,没有关于疗效的结论可以直接推断出来。
Characteristics and Outcomes of Patients Receiving Volatile Anesthetics in Near-Fatal Asthma: A Retrospective Observational Cohort Study.
Importance and objectives: Inhaled volatile anesthetics are employed as rescue therapy in near-fatal asthma, despite limited evidence. This study aims to describe the characteristics, management, and outcomes of mechanically ventilated adult patients with near-fatal asthma, stratified by the use of volatile anesthetic therapy.
Setting: Tertiary critical care and extracorporeal membrane oxygenation (ECMO) unit.
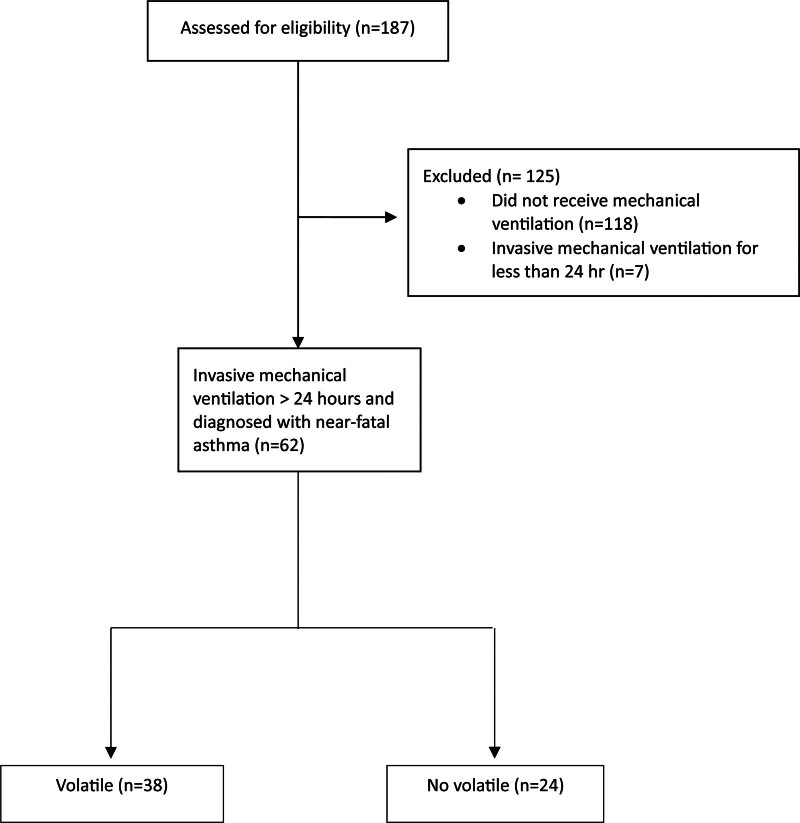
Participants: Adults 16 years old or older receiving mechanical ventilation (MV) for greater than or equal to 24 hours and/or ECMO between January 2016 and August 2023 for near-fatal asthma.
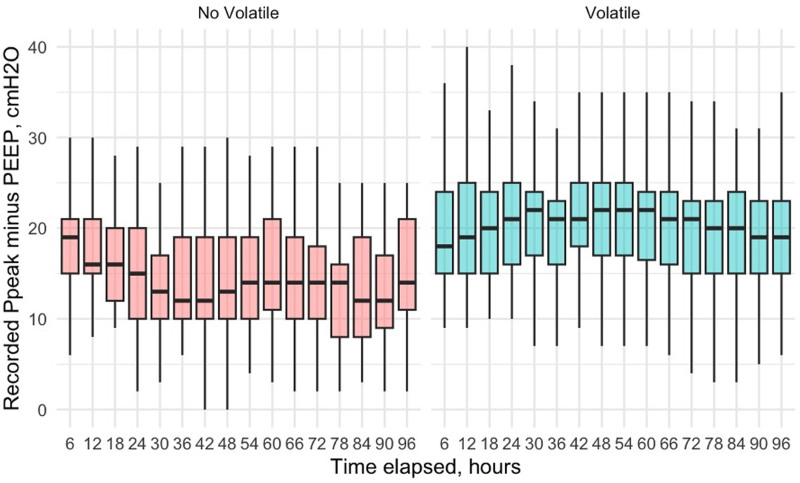
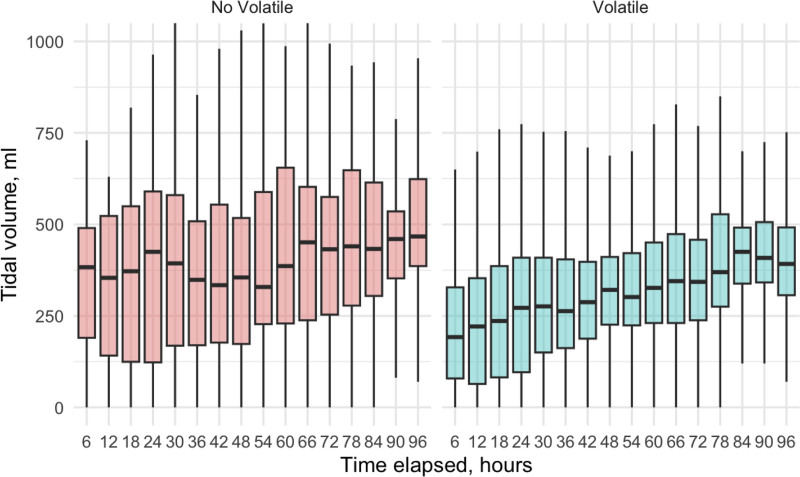
Main outcomes and measures: We recorded demographics, disease severity tidal volumes, and ventilator settings, by treatment over the first 100 hours. Outcomes were duration of ECMO and MV, ICU length of stay, 90-day mortality, and adverse drug reaction.
Results: Sixty-two patients were included (62.9% female), with a median (interquartile range [IQR]) age of 45 years (29-51 yr). Median (IQR) pH 7.13 (6.93-7.23), Paco2 12.9 kPa (8.7-16.2 kPa), and tidal volume 178 mL (50-300 mL). Most patients received IV bronchodilators and 32 (51.6%) required ECMO. Thirty-eight patients (61.3%) were treated with volatile anesthetics. Volatile patients had worse ventilation and blood gas parameters before treatment, more barotrauma, and were more likely to be receiving ECMO. Despite this, improvements in tidal volume occurred in the volatile group (mean increase, 204 mL [83.9%]; 95% CI, 110-298; p < 0.001). Median (IQR) duration of MV and ICU length of stay in volatile and no volatile patients were 10 days (8-16 d) vs. 5 days (3-10 d; p = 0.001) and 15 days (13-20 d) vs. 9 days (7-14 d; p = 0.001), respectively. ICU and 90-day mortality in volatile and no volatile patients were 5.3% vs. 4.2%.
Conclusions and relevance: The use of inhaled volatile anesthetics for near-fatal asthma, including during ECMO, appears to be feasible and safe, and with favorable clinical outcomes; however, no conclusions regarding efficacy can be directly inferred.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


