Sandra Campos, Maria Angeles Ballesteros, Emilio Rodrigo, Covadonga López Del Moral, Félix Campos-Juanatey, Borja Suberviola, Lucía García-Alcalde, Aurora Amaya, Beatriz Domínguez-Gil, Juan Carlos Ruiz-San Millan, Eduardo Miñambres
{"title":"新的供体选择标准在血液循环确定死亡后导致无控制捐赠肾脏的最佳结果。","authors":"Sandra Campos, Maria Angeles Ballesteros, Emilio Rodrigo, Covadonga López Del Moral, Félix Campos-Juanatey, Borja Suberviola, Lucía García-Alcalde, Aurora Amaya, Beatriz Domínguez-Gil, Juan Carlos Ruiz-San Millan, Eduardo Miñambres","doi":"10.1097/TXD.0000000000001790","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of our study is to share our experience with uncontrolled donation after the circulatory determination of death (uDCDD) kidney transplantation and to propose updated donor selection criteria for uDCDD programs.</p><p><strong>Methods: </strong>A prospective study comparing kidney recipients of grafts from local uDCDD donors with recipients of grafts from local standard criteria donors after the neurological determination of death (DNDD) between 2013 and 2024. Donor acceptance was determined using a combination of 3 factors: donor age, no-flow period, and warm ischemic time (WIT). Normothermic regional perfusion was the preservation method in uDCDD cases.</p><p><strong>Results: </strong>The study included 43 kidney recipients from uDCDD donors and 80 controls. The median no-flow period was 10 min (interquartile range, 5-13), and the median WIT was 101 min (interquartile range, 86-118). The incidence of delayed graft function was significantly higher in the uDCDD group (46.5% versus 21.3%; <i>P</i> = 0.004), although no significant difference was observed in primary nonfunction rates (2.3% versus 0%; <i>P</i> = 0.35). Long-term outcomes, including serum creatinine levels and estimated glomerular filtration rate at 5 y, were similar in both groups. Graft survival rates at 1 y (95.3% versus 100%) and 5 y (92.1% versus 95%) showed no significant differences between the uDCDD and the DNDD groups. Multivariate analysis revealed that uDCDD kidney recipients did not have a higher risk of graft loss.</p><p><strong>Conclusions: </strong>Kidney transplantation from uDCDD donors is a viable option, yielding outcomes comparable with those from standard DNDD donors. Strict donor selection criteria and efforts to minimize WIT are essential to achieving optimal long-term results.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 5","pages":"e1790"},"PeriodicalIF":1.9000,"publicationDate":"2025-04-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12310195/pdf/","citationCount":"0","resultStr":"{\"title\":\"New Donor Selection Criteria Result in Optimal Outcomes of Kidneys from Uncontrolled Donation After the Circulatory Determination of Death.\",\"authors\":\"Sandra Campos, Maria Angeles Ballesteros, Emilio Rodrigo, Covadonga López Del Moral, Félix Campos-Juanatey, Borja Suberviola, Lucía García-Alcalde, Aurora Amaya, Beatriz Domínguez-Gil, Juan Carlos Ruiz-San Millan, Eduardo Miñambres\",\"doi\":\"10.1097/TXD.0000000000001790\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The aim of our study is to share our experience with uncontrolled donation after the circulatory determination of death (uDCDD) kidney transplantation and to propose updated donor selection criteria for uDCDD programs.</p><p><strong>Methods: </strong>A prospective study comparing kidney recipients of grafts from local uDCDD donors with recipients of grafts from local standard criteria donors after the neurological determination of death (DNDD) between 2013 and 2024. Donor acceptance was determined using a combination of 3 factors: donor age, no-flow period, and warm ischemic time (WIT). Normothermic regional perfusion was the preservation method in uDCDD cases.</p><p><strong>Results: </strong>The study included 43 kidney recipients from uDCDD donors and 80 controls. The median no-flow period was 10 min (interquartile range, 5-13), and the median WIT was 101 min (interquartile range, 86-118). The incidence of delayed graft function was significantly higher in the uDCDD group (46.5% versus 21.3%; <i>P</i> = 0.004), although no significant difference was observed in primary nonfunction rates (2.3% versus 0%; <i>P</i> = 0.35). Long-term outcomes, including serum creatinine levels and estimated glomerular filtration rate at 5 y, were similar in both groups. Graft survival rates at 1 y (95.3% versus 100%) and 5 y (92.1% versus 95%) showed no significant differences between the uDCDD and the DNDD groups. Multivariate analysis revealed that uDCDD kidney recipients did not have a higher risk of graft loss.</p><p><strong>Conclusions: </strong>Kidney transplantation from uDCDD donors is a viable option, yielding outcomes comparable with those from standard DNDD donors. Strict donor selection criteria and efforts to minimize WIT are essential to achieving optimal long-term results.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"11 5\",\"pages\":\"e1790\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-04-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12310195/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001790\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001790","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
摘要
背景:本研究的目的是分享我们在循环确定死亡(uDCDD)肾移植后无控制捐赠的经验,并为uDCDD项目提出更新的供体选择标准。方法:一项前瞻性研究,比较2013年至2024年间当地uDCDD供者肾移植受者和当地标准标准供者肾移植受者在神经学判断死亡(DNDD)后的肾移植受者。供体接受度由供体年龄、无血流期和热缺血时间(WIT) 3个因素综合决定。常温局部灌注是uDCDD的保存方法。结果:该研究包括43名来自uDCDD供者的肾受体和80名对照组。无流期中位数为10 min(四分位数范围5-13),WIT中位数为101 min(四分位数范围86-118)。uDCDD组移植物功能延迟的发生率显著高于前者(46.5% vs 21.3%;P = 0.004),但未观察到原发性功能丧失率的显著差异(2.3% vs 0%;p = 0.35)。两组的长期结果,包括血清肌酐水平和5岁时肾小球滤过率的估计,相似。1年(95.3%对100%)和5年(92.1%对95%)的移植物存活率在uDCDD组和DNDD组之间没有显著差异。多变量分析显示,uDCDD肾受者没有更高的移植物丢失风险。结论:来自uDCDD供者的肾移植是一种可行的选择,其结果与来自标准ddd供者的结果相当。严格的捐赠者选择标准和尽量减少WIT的努力对于实现最佳的长期结果至关重要。
New Donor Selection Criteria Result in Optimal Outcomes of Kidneys from Uncontrolled Donation After the Circulatory Determination of Death.
Background: The aim of our study is to share our experience with uncontrolled donation after the circulatory determination of death (uDCDD) kidney transplantation and to propose updated donor selection criteria for uDCDD programs.
Methods: A prospective study comparing kidney recipients of grafts from local uDCDD donors with recipients of grafts from local standard criteria donors after the neurological determination of death (DNDD) between 2013 and 2024. Donor acceptance was determined using a combination of 3 factors: donor age, no-flow period, and warm ischemic time (WIT). Normothermic regional perfusion was the preservation method in uDCDD cases.
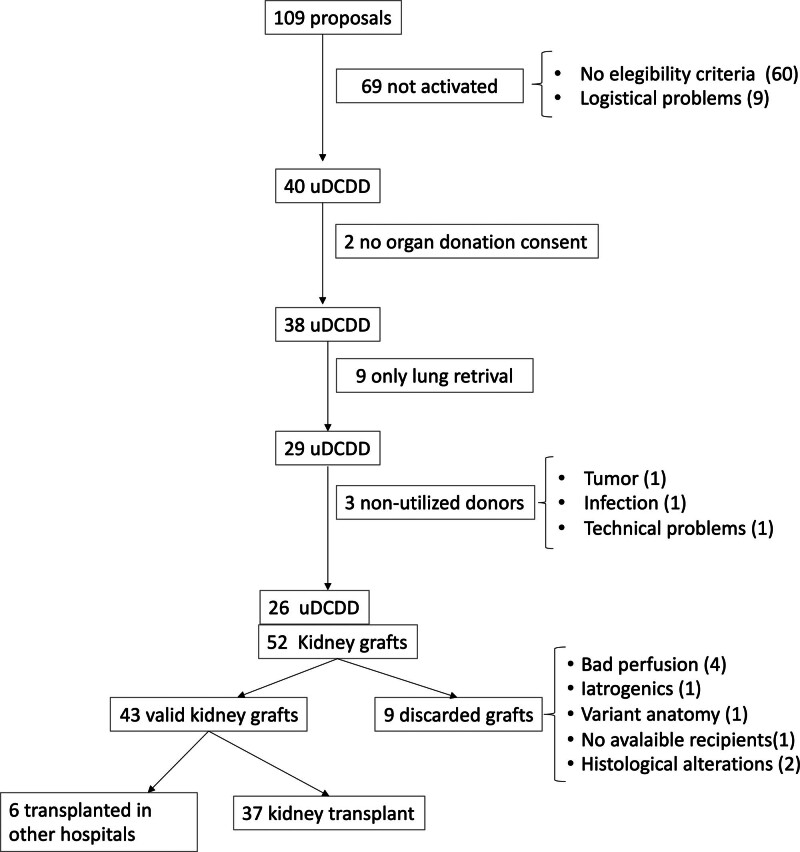
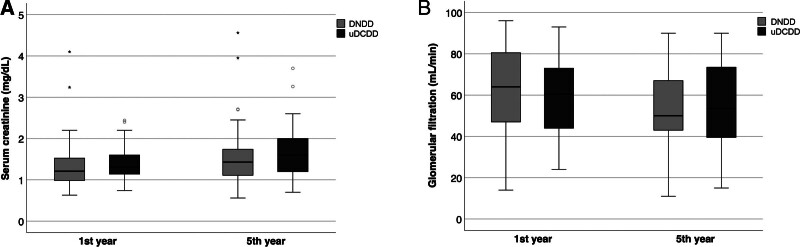
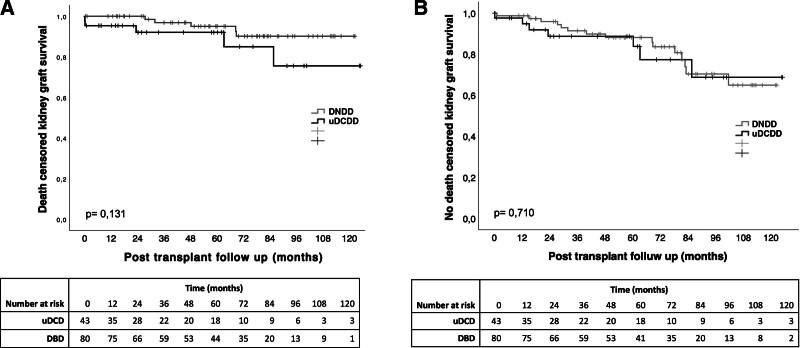
Results: The study included 43 kidney recipients from uDCDD donors and 80 controls. The median no-flow period was 10 min (interquartile range, 5-13), and the median WIT was 101 min (interquartile range, 86-118). The incidence of delayed graft function was significantly higher in the uDCDD group (46.5% versus 21.3%; P = 0.004), although no significant difference was observed in primary nonfunction rates (2.3% versus 0%; P = 0.35). Long-term outcomes, including serum creatinine levels and estimated glomerular filtration rate at 5 y, were similar in both groups. Graft survival rates at 1 y (95.3% versus 100%) and 5 y (92.1% versus 95%) showed no significant differences between the uDCDD and the DNDD groups. Multivariate analysis revealed that uDCDD kidney recipients did not have a higher risk of graft loss.
Conclusions: Kidney transplantation from uDCDD donors is a viable option, yielding outcomes comparable with those from standard DNDD donors. Strict donor selection criteria and efforts to minimize WIT are essential to achieving optimal long-term results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


