Lana Hasan, Lalithaa Thirunavukarasu Murugan, Eileen Hsich, Michael Zhen-Yu Tong, Kyle D. Brizendine
{"title":"原位心脏移植患者侵袭性真菌感染:现代发病率及危险因素","authors":"Lana Hasan, Lalithaa Thirunavukarasu Murugan, Eileen Hsich, Michael Zhen-Yu Tong, Kyle D. Brizendine","doi":"10.1111/ctr.70248","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Invasive fungal infections (IFI) post-orthotopic heart transplant (OHT) have not been well studied due to limited information in large databases. The goal of the study is to describe the incidence and risk factors for IFI.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>In this retrospective cohort study, we analyzed risk factors associated with IFI among OHT recipients in our center in the period 2010–2020. Patients were divided into two groups for comparison: IFI within the first year after transplant, and no IFI. We compared the groups to determine independent risk factors for IFI.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Out of 548 included patients, 29 patients experienced 29 IFI (incidence = 5.3%; 95% CI 3.7–7.5). Median (interquartile range) time to IFI was 44 days (10–238.5). <i>Candida</i> was the most identified pathogen (51%), followed by <i>Aspergillus</i> (27%) and <i>Cryptococcus</i> (9%). In multivariable logistic regression analyses, pretransplant fungal colonization/infection (odds ratio, [OR] 27, 95% CI 1.2–315), post-transplant reoperation (OR 5.8, 95% CI 2.2–15), and extracorporeal membrane oxygenation (ECMO) (OR 3.1, 95% CI 1.1–9.0) were associated with increased odds of IFI. Compared to patients without IFI, 1-year survival of patients with IFI was significantly worse (76 vs. 97%, <i>p</i> < 0.01).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>We conclude there are specific, identifiable risk factors during the pre- and post-transplant periods associated with increased odds of IFI. These merit study of targeted antifungal prophylaxis with agents offering broad yeast and mold activity in OHT patients with certain risk factors.</p>\n </section>\n </div>","PeriodicalId":10467,"journal":{"name":"Clinical Transplantation","volume":"39 8","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.70248","citationCount":"0","resultStr":"{\"title\":\"Invasive Fungal Infections in Orthotopic Heart Transplant Patients: Incidence and Risk Factors in the Modern Era\",\"authors\":\"Lana Hasan, Lalithaa Thirunavukarasu Murugan, Eileen Hsich, Michael Zhen-Yu Tong, Kyle D. Brizendine\",\"doi\":\"10.1111/ctr.70248\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Invasive fungal infections (IFI) post-orthotopic heart transplant (OHT) have not been well studied due to limited information in large databases. The goal of the study is to describe the incidence and risk factors for IFI.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>In this retrospective cohort study, we analyzed risk factors associated with IFI among OHT recipients in our center in the period 2010–2020. Patients were divided into two groups for comparison: IFI within the first year after transplant, and no IFI. We compared the groups to determine independent risk factors for IFI.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Out of 548 included patients, 29 patients experienced 29 IFI (incidence = 5.3%; 95% CI 3.7–7.5). Median (interquartile range) time to IFI was 44 days (10–238.5). <i>Candida</i> was the most identified pathogen (51%), followed by <i>Aspergillus</i> (27%) and <i>Cryptococcus</i> (9%). In multivariable logistic regression analyses, pretransplant fungal colonization/infection (odds ratio, [OR] 27, 95% CI 1.2–315), post-transplant reoperation (OR 5.8, 95% CI 2.2–15), and extracorporeal membrane oxygenation (ECMO) (OR 3.1, 95% CI 1.1–9.0) were associated with increased odds of IFI. Compared to patients without IFI, 1-year survival of patients with IFI was significantly worse (76 vs. 97%, <i>p</i> < 0.01).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>We conclude there are specific, identifiable risk factors during the pre- and post-transplant periods associated with increased odds of IFI. These merit study of targeted antifungal prophylaxis with agents offering broad yeast and mold activity in OHT patients with certain risk factors.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10467,\"journal\":{\"name\":\"Clinical Transplantation\",\"volume\":\"39 8\",\"pages\":\"\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ctr.70248\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70248\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Transplantation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ctr.70248","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
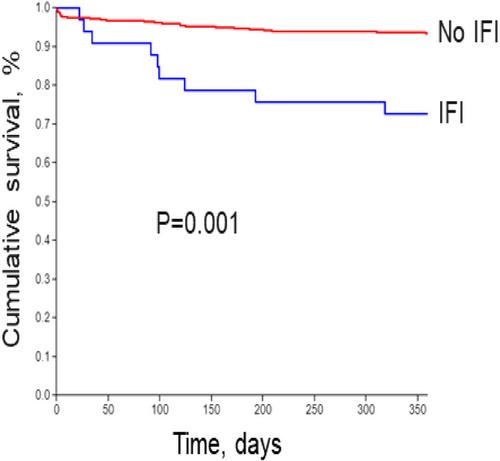
背景:由于大型数据库信息有限,原位心脏移植(OHT)后侵袭性真菌感染(IFI)尚未得到很好的研究。本研究的目的是描述IFI的发生率和危险因素。方法在这项回顾性队列研究中,我们分析了本中心2010-2020年期间OHT受者中IFI相关的危险因素。将患者分为两组进行比较:移植后一年内进行IFI和未进行IFI。我们比较两组以确定IFI的独立危险因素。结果548例患者中,29例患者发生29次IFI(发生率为5.3%;95% ci 3.7-7.5)。到IFI的中位时间(四分位数间距)为44天(10-238.5天)。念珠菌是鉴定最多的病原菌(51%),其次是曲霉(27%)和隐球菌(9%)。在多变量logistic回归分析中,移植前真菌定植/感染(比值比[OR] 27, 95% CI 1.2-315)、移植后再手术(比值比[OR] 5.8, 95% CI 2.2-15)和体外膜氧合(ECMO)(比值比3.1,95% CI 1.1-9.0)与IFI的发生率增加相关。与没有IFI的患者相比,IFI患者的1年生存率明显较差(76% vs. 97%, p <;0.01)。我们得出结论,在移植前和移植后期间,存在与IFI发生率增加相关的特定、可识别的危险因素。这些值得对具有一定危险因素的OHT患者使用具有广泛酵母和霉菌活性的药物进行针对性的抗真菌预防研究。
Invasive Fungal Infections in Orthotopic Heart Transplant Patients: Incidence and Risk Factors in the Modern Era
Background
Invasive fungal infections (IFI) post-orthotopic heart transplant (OHT) have not been well studied due to limited information in large databases. The goal of the study is to describe the incidence and risk factors for IFI.
Methods
In this retrospective cohort study, we analyzed risk factors associated with IFI among OHT recipients in our center in the period 2010–2020. Patients were divided into two groups for comparison: IFI within the first year after transplant, and no IFI. We compared the groups to determine independent risk factors for IFI.
Results
Out of 548 included patients, 29 patients experienced 29 IFI (incidence = 5.3%; 95% CI 3.7–7.5). Median (interquartile range) time to IFI was 44 days (10–238.5). Candida was the most identified pathogen (51%), followed by Aspergillus (27%) and Cryptococcus (9%). In multivariable logistic regression analyses, pretransplant fungal colonization/infection (odds ratio, [OR] 27, 95% CI 1.2–315), post-transplant reoperation (OR 5.8, 95% CI 2.2–15), and extracorporeal membrane oxygenation (ECMO) (OR 3.1, 95% CI 1.1–9.0) were associated with increased odds of IFI. Compared to patients without IFI, 1-year survival of patients with IFI was significantly worse (76 vs. 97%, p < 0.01).
Conclusions
We conclude there are specific, identifiable risk factors during the pre- and post-transplant periods associated with increased odds of IFI. These merit study of targeted antifungal prophylaxis with agents offering broad yeast and mold activity in OHT patients with certain risk factors.
期刊介绍:
Clinical Transplantation: The Journal of Clinical and Translational Research aims to serve as a channel of rapid communication for all those involved in the care of patients who require, or have had, organ or tissue transplants, including: kidney, intestine, liver, pancreas, islets, heart, heart valves, lung, bone marrow, cornea, skin, bone, and cartilage, viable or stored.
Published monthly, Clinical Transplantation’s scope is focused on the complete spectrum of present transplant therapies, as well as also those that are experimental or may become possible in future. Topics include:
Immunology and immunosuppression;
Patient preparation;
Social, ethical, and psychological issues;
Complications, short- and long-term results;
Artificial organs;
Donation and preservation of organ and tissue;
Translational studies;
Advances in tissue typing;
Updates on transplant pathology;.
Clinical and translational studies are particularly welcome, as well as focused reviews. Full-length papers and short communications are invited. Clinical reviews are encouraged, as well as seminal papers in basic science which might lead to immediate clinical application. Prominence is regularly given to the results of cooperative surveys conducted by the organ and tissue transplant registries.
Clinical Transplantation: The Journal of Clinical and Translational Research is essential reading for clinicians and researchers in the diverse field of transplantation: surgeons; clinical immunologists; cryobiologists; hematologists; gastroenterologists; hepatologists; pulmonologists; nephrologists; cardiologists; and endocrinologists. It will also be of interest to sociologists, psychologists, research workers, and to all health professionals whose combined efforts will improve the prognosis of transplant recipients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


