Ronen Arai, Adria Condino, Bincy P Abraham, Stephen B Hanauer, Udayakumar Navaneethan, Donald Lum, Syed A Hassan, Timothy Ritter, Esther A Torres, David Ziring, Harry Bray, Thierry Dervieux, Patricia Aragon Han, Terrence A Barrett
{"title":"精确指导给药对炎症性肠病临床决策和医疗保健利用的影响:一项回顾性测试前/测试后的真实世界研究","authors":"Ronen Arai, Adria Condino, Bincy P Abraham, Stephen B Hanauer, Udayakumar Navaneethan, Donald Lum, Syed A Hassan, Timothy Ritter, Esther A Torres, David Ziring, Harry Bray, Thierry Dervieux, Patricia Aragon Han, Terrence A Barrett","doi":"10.1093/crocol/otaf044","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Precision-guided dosing (PGD) is a personalized tool that optimizes clinical decision-making in the treatment of inflammatory bowel disease (IBD) with infliximab (IFX) and its biosimilars. PGD employs nonlinear mixed-effect models using patient-specific pharmacokinetic parameters to predict infliximab trough concentrations without the need to wait until the actual trough measurement. This approach calculates patient-specific clearance (CL) and provides tailored IFX dosing and administration intervals aimed at achieving target trough levels. Implementing PGD can enhance treatment outcomes in IBD patients and may potentially reduce healthcare expenditures.</p><p><strong>Methods: </strong>We conducted a multicenter, retrospective study as a follow up to our previous clinical experience program (CEP). We aimed to evaluate the impact of PGD on clinical decision-making, patient outcomes, healthcare utilization, and expenditures. Treatment decisions included: IFX dose intensification, reduction, discontinuation, or continuation. Disease activity and healthcare resource utilization and costs in the 12 months pre- and post-test were compared. Disease activity was measured using the physician global assessment (PGA) as follows: remission (0), mild (1), moderate (2), and severe (3). Costs were calculated based on modeling pre-established literature data.</p><p><strong>Results: </strong>Analysis of data from 82 patients across 7 states and Puerto Rico showed that PGD-driven therapeutic decision making led to IFX treatment intensification (27%) or discontinuation (7%) in patients with low forecasted trough IFX concentrations, high clearance, and presence of antidrug antibody. Conversely, IFX dosage was reduced (18%) or unchanged (48%) for patients with high IFX concentrations and low clearance. There was a significant association between forecasted trough IFX levels and treatment modifications (<i>P</i> < .001). High clearance (> 0.294 L/day) was significantly associated with therapy intensification (OR 6.22, 95% CI: 2.19-19.8; <i>P</i> < .001). Following PGD, disease activity improved significantly (observed mean difference in physician global assessment: 0.378, <i>P</i> = 0.008) and healthcare resource utilization decreased. Across the entire patient population, hospitalizations decreased from 30 events pretest to 5 events posttest (<i>P</i> < .001), leading to overall cost saving.</p><p><strong>Conclusions: </strong>HCPs used the PGD test to guide treatment decisions. PGD-driven optimization of IFX therapy led to improved patient outcomes, lower healthcare utilization, and cost savings.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"7 3","pages":"otaf044"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305531/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Precision-Guided Dosing on Clinical Decision-Making and Health Care Utilization in Inflammatory Bowel Disease: A Retrospective Pretest/Posttest Real-World Study.\",\"authors\":\"Ronen Arai, Adria Condino, Bincy P Abraham, Stephen B Hanauer, Udayakumar Navaneethan, Donald Lum, Syed A Hassan, Timothy Ritter, Esther A Torres, David Ziring, Harry Bray, Thierry Dervieux, Patricia Aragon Han, Terrence A Barrett\",\"doi\":\"10.1093/crocol/otaf044\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Precision-guided dosing (PGD) is a personalized tool that optimizes clinical decision-making in the treatment of inflammatory bowel disease (IBD) with infliximab (IFX) and its biosimilars. PGD employs nonlinear mixed-effect models using patient-specific pharmacokinetic parameters to predict infliximab trough concentrations without the need to wait until the actual trough measurement. This approach calculates patient-specific clearance (CL) and provides tailored IFX dosing and administration intervals aimed at achieving target trough levels. Implementing PGD can enhance treatment outcomes in IBD patients and may potentially reduce healthcare expenditures.</p><p><strong>Methods: </strong>We conducted a multicenter, retrospective study as a follow up to our previous clinical experience program (CEP). We aimed to evaluate the impact of PGD on clinical decision-making, patient outcomes, healthcare utilization, and expenditures. Treatment decisions included: IFX dose intensification, reduction, discontinuation, or continuation. Disease activity and healthcare resource utilization and costs in the 12 months pre- and post-test were compared. Disease activity was measured using the physician global assessment (PGA) as follows: remission (0), mild (1), moderate (2), and severe (3). Costs were calculated based on modeling pre-established literature data.</p><p><strong>Results: </strong>Analysis of data from 82 patients across 7 states and Puerto Rico showed that PGD-driven therapeutic decision making led to IFX treatment intensification (27%) or discontinuation (7%) in patients with low forecasted trough IFX concentrations, high clearance, and presence of antidrug antibody. Conversely, IFX dosage was reduced (18%) or unchanged (48%) for patients with high IFX concentrations and low clearance. There was a significant association between forecasted trough IFX levels and treatment modifications (<i>P</i> < .001). High clearance (> 0.294 L/day) was significantly associated with therapy intensification (OR 6.22, 95% CI: 2.19-19.8; <i>P</i> < .001). Following PGD, disease activity improved significantly (observed mean difference in physician global assessment: 0.378, <i>P</i> = 0.008) and healthcare resource utilization decreased. Across the entire patient population, hospitalizations decreased from 30 events pretest to 5 events posttest (<i>P</i> < .001), leading to overall cost saving.</p><p><strong>Conclusions: </strong>HCPs used the PGD test to guide treatment decisions. PGD-driven optimization of IFX therapy led to improved patient outcomes, lower healthcare utilization, and cost savings.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":\"7 3\",\"pages\":\"otaf044\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-06-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305531/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otaf044\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otaf044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
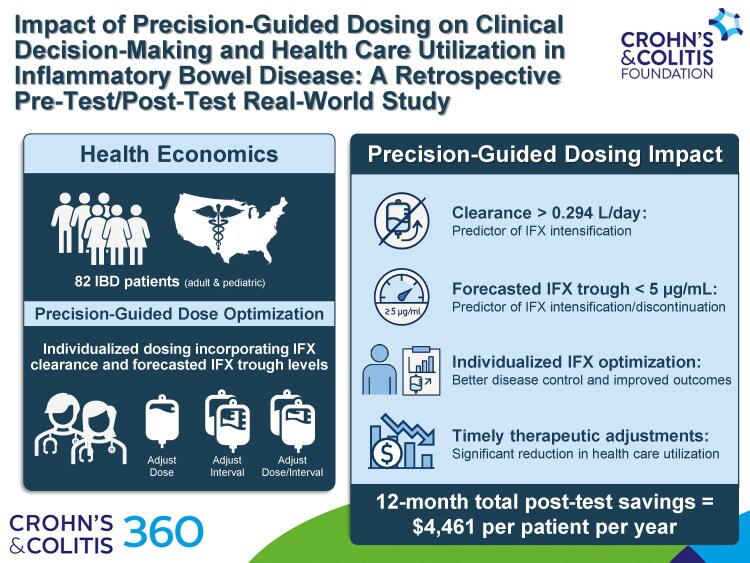
Impact of Precision-Guided Dosing on Clinical Decision-Making and Health Care Utilization in Inflammatory Bowel Disease: A Retrospective Pretest/Posttest Real-World Study.
Background: Precision-guided dosing (PGD) is a personalized tool that optimizes clinical decision-making in the treatment of inflammatory bowel disease (IBD) with infliximab (IFX) and its biosimilars. PGD employs nonlinear mixed-effect models using patient-specific pharmacokinetic parameters to predict infliximab trough concentrations without the need to wait until the actual trough measurement. This approach calculates patient-specific clearance (CL) and provides tailored IFX dosing and administration intervals aimed at achieving target trough levels. Implementing PGD can enhance treatment outcomes in IBD patients and may potentially reduce healthcare expenditures.
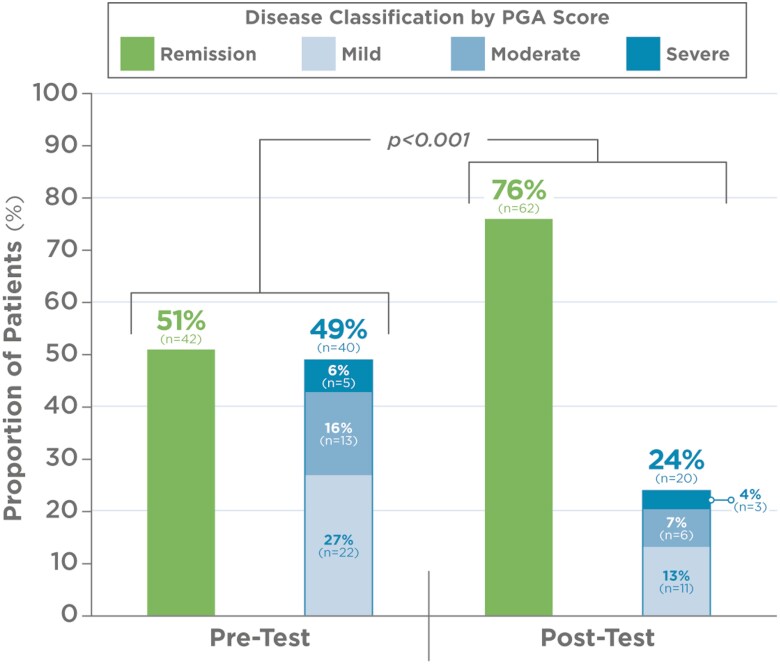
Methods: We conducted a multicenter, retrospective study as a follow up to our previous clinical experience program (CEP). We aimed to evaluate the impact of PGD on clinical decision-making, patient outcomes, healthcare utilization, and expenditures. Treatment decisions included: IFX dose intensification, reduction, discontinuation, or continuation. Disease activity and healthcare resource utilization and costs in the 12 months pre- and post-test were compared. Disease activity was measured using the physician global assessment (PGA) as follows: remission (0), mild (1), moderate (2), and severe (3). Costs were calculated based on modeling pre-established literature data.
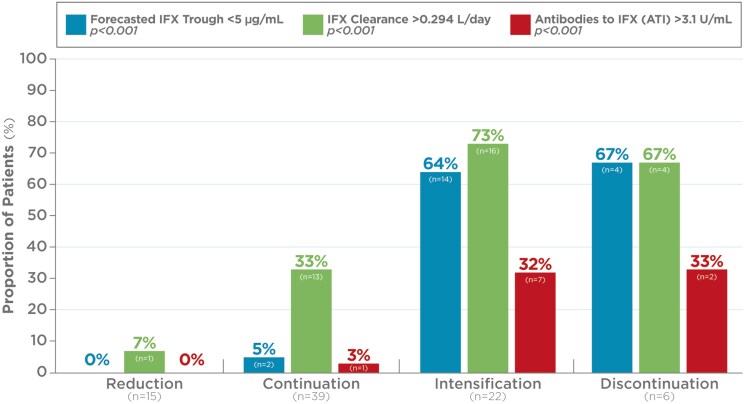
Results: Analysis of data from 82 patients across 7 states and Puerto Rico showed that PGD-driven therapeutic decision making led to IFX treatment intensification (27%) or discontinuation (7%) in patients with low forecasted trough IFX concentrations, high clearance, and presence of antidrug antibody. Conversely, IFX dosage was reduced (18%) or unchanged (48%) for patients with high IFX concentrations and low clearance. There was a significant association between forecasted trough IFX levels and treatment modifications (P < .001). High clearance (> 0.294 L/day) was significantly associated with therapy intensification (OR 6.22, 95% CI: 2.19-19.8; P < .001). Following PGD, disease activity improved significantly (observed mean difference in physician global assessment: 0.378, P = 0.008) and healthcare resource utilization decreased. Across the entire patient population, hospitalizations decreased from 30 events pretest to 5 events posttest (P < .001), leading to overall cost saving.
Conclusions: HCPs used the PGD test to guide treatment decisions. PGD-driven optimization of IFX therapy led to improved patient outcomes, lower healthcare utilization, and cost savings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


