Soraya Benamar, Cédric Lukas, Claire Daien, Cécile Gaujoux-Viala, Laure Gossec, Anne-Christine Rat, Bernard Combe, Jacques Morel
{"title":"多药治疗早期类风湿关节炎:法国一项多中心前瞻性队列研究对治疗反应和不良事件风险的影响。","authors":"Soraya Benamar, Cédric Lukas, Claire Daien, Cécile Gaujoux-Viala, Laure Gossec, Anne-Christine Rat, Bernard Combe, Jacques Morel","doi":"10.1002/acr2.70066","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The objective of this study was to assess whether polypharmacy (PP) was associated with treatment response and serious adverse events (SAEs) in early rheumatoid arthritis (RA). Additionally, we aimed to investigate whether PP could serve as a surrogate marker for comorbidities.</p><p><strong>Methods: </strong>We used data from the French cohort ESPOIR, a prospective study of early RA. PP was defined as a categorical variable stratified into two or three categories according to median of distribution in the cohort. A logistic regression model was used. We assessed the occurrence of SAEs (severe infections, hospitalizations, deaths) throughout a 10-year follow-up period.</p><p><strong>Results: </strong>The proportion of patients who achieved DAS 28 remission (REM) one year after the initiation of the first disease-modifying antirheumatic drug (DMARD) was 32.1% in the PP group versus 67.9% in the non-PP group (P = 0.07) from 497 patients included. At five years, the proportion with REM was 45.0% in the PP group versus 56.3% in the non-PP group (P = 0.03). Patients taking two or more medications (excluding RA therapy) had a 40% lower likelihood of achieving REM at five years (adjusted odds ratio [OR] 0.60 [95% confidence interval (CI) 0.38-0.94], P = 0.03). At 10 years, patients receiving multiple medications had a 43% lower probability of achieving REM (adjusted OR 0.57 [95% CI 0.34-0.94], P = 0.02). The incidence of SAEs was 61 per 1,000 person-years. Among patients who developed SAEs, 86.4% were in the PP group and 49.8% were in the non-PP group (P = 0.03).</p><p><strong>Conclusion: </strong>PP is associated with a poorer treatment response and increased risk of SAEs. PP may serve as a good surrogate marker of comorbidities in epidemiologic studies.</p>","PeriodicalId":93845,"journal":{"name":"ACR open rheumatology","volume":"7 8","pages":"e70066"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305454/pdf/","citationCount":"0","resultStr":"{\"title\":\"Polypharmacy in Early Rheumatoid Arthritis: Impact on Treatment Response and Adverse Event Risk in a multicenter French prospective cohort study.\",\"authors\":\"Soraya Benamar, Cédric Lukas, Claire Daien, Cécile Gaujoux-Viala, Laure Gossec, Anne-Christine Rat, Bernard Combe, Jacques Morel\",\"doi\":\"10.1002/acr2.70066\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The objective of this study was to assess whether polypharmacy (PP) was associated with treatment response and serious adverse events (SAEs) in early rheumatoid arthritis (RA). Additionally, we aimed to investigate whether PP could serve as a surrogate marker for comorbidities.</p><p><strong>Methods: </strong>We used data from the French cohort ESPOIR, a prospective study of early RA. PP was defined as a categorical variable stratified into two or three categories according to median of distribution in the cohort. A logistic regression model was used. We assessed the occurrence of SAEs (severe infections, hospitalizations, deaths) throughout a 10-year follow-up period.</p><p><strong>Results: </strong>The proportion of patients who achieved DAS 28 remission (REM) one year after the initiation of the first disease-modifying antirheumatic drug (DMARD) was 32.1% in the PP group versus 67.9% in the non-PP group (P = 0.07) from 497 patients included. At five years, the proportion with REM was 45.0% in the PP group versus 56.3% in the non-PP group (P = 0.03). Patients taking two or more medications (excluding RA therapy) had a 40% lower likelihood of achieving REM at five years (adjusted odds ratio [OR] 0.60 [95% confidence interval (CI) 0.38-0.94], P = 0.03). At 10 years, patients receiving multiple medications had a 43% lower probability of achieving REM (adjusted OR 0.57 [95% CI 0.34-0.94], P = 0.02). The incidence of SAEs was 61 per 1,000 person-years. Among patients who developed SAEs, 86.4% were in the PP group and 49.8% were in the non-PP group (P = 0.03).</p><p><strong>Conclusion: </strong>PP is associated with a poorer treatment response and increased risk of SAEs. PP may serve as a good surrogate marker of comorbidities in epidemiologic studies.</p>\",\"PeriodicalId\":93845,\"journal\":{\"name\":\"ACR open rheumatology\",\"volume\":\"7 8\",\"pages\":\"e70066\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12305454/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR open rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.70066\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR open rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.70066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究的目的是评估多种药物(PP)是否与早期类风湿关节炎(RA)的治疗反应和严重不良事件(SAEs)相关。此外,我们的目的是研究PP是否可以作为合并症的替代标志物。方法:我们使用来自法国队列ESPOIR的数据,这是一项早期RA的前瞻性研究。PP被定义为一个分类变量,根据队列中分布的中位数分为两个或三个类别。采用logistic回归模型。我们评估了10年随访期间SAEs(严重感染、住院、死亡)的发生情况。结果:在纳入的497例患者中,PP组在首次使用改善疾病的抗风湿药物(DMARD)一年后达到DAS 28缓解(REM)的比例为32.1%,而非PP组为67.9% (P = 0.07)。5年时,PP组有REM的比例为45.0%,非PP组为56.3% (P = 0.03)。服用两种或两种以上药物(不包括RA治疗)的患者在5年内达到REM的可能性降低40%(校正优势比[or] 0.60[95%可信区间(CI) 0.38-0.94], P = 0.03)。在10年时,接受多种药物治疗的患者达到REM的概率降低43%(调整后OR为0.57 [95% CI 0.34-0.94], P = 0.02)。急性呼吸道感染的发生率为61 / 1000人年。发生SAEs的患者中,PP组占86.4%,非PP组占49.8% (P = 0.03)。结论:PP与较差的治疗反应和增加的SAEs风险相关。在流行病学研究中,PP可作为合并症的良好替代指标。
Polypharmacy in Early Rheumatoid Arthritis: Impact on Treatment Response and Adverse Event Risk in a multicenter French prospective cohort study.
Objective: The objective of this study was to assess whether polypharmacy (PP) was associated with treatment response and serious adverse events (SAEs) in early rheumatoid arthritis (RA). Additionally, we aimed to investigate whether PP could serve as a surrogate marker for comorbidities.
Methods: We used data from the French cohort ESPOIR, a prospective study of early RA. PP was defined as a categorical variable stratified into two or three categories according to median of distribution in the cohort. A logistic regression model was used. We assessed the occurrence of SAEs (severe infections, hospitalizations, deaths) throughout a 10-year follow-up period.
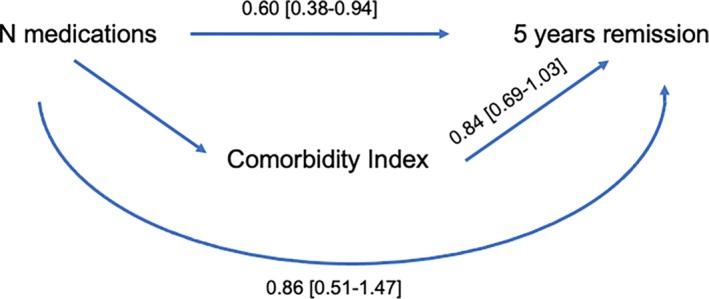
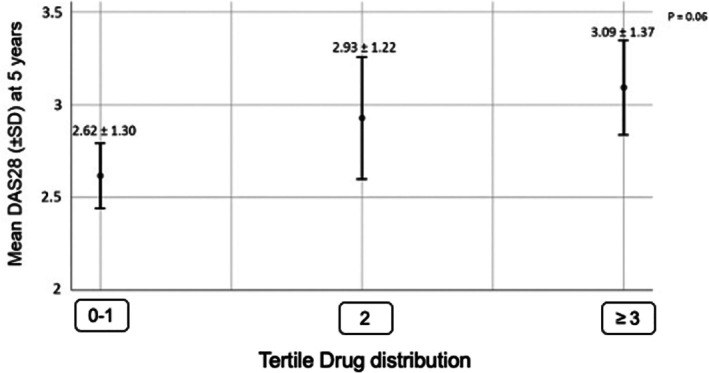
Results: The proportion of patients who achieved DAS 28 remission (REM) one year after the initiation of the first disease-modifying antirheumatic drug (DMARD) was 32.1% in the PP group versus 67.9% in the non-PP group (P = 0.07) from 497 patients included. At five years, the proportion with REM was 45.0% in the PP group versus 56.3% in the non-PP group (P = 0.03). Patients taking two or more medications (excluding RA therapy) had a 40% lower likelihood of achieving REM at five years (adjusted odds ratio [OR] 0.60 [95% confidence interval (CI) 0.38-0.94], P = 0.03). At 10 years, patients receiving multiple medications had a 43% lower probability of achieving REM (adjusted OR 0.57 [95% CI 0.34-0.94], P = 0.02). The incidence of SAEs was 61 per 1,000 person-years. Among patients who developed SAEs, 86.4% were in the PP group and 49.8% were in the non-PP group (P = 0.03).
Conclusion: PP is associated with a poorer treatment response and increased risk of SAEs. PP may serve as a good surrogate marker of comorbidities in epidemiologic studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


