Lucrecia M Burgos, Lucía Campos Cervera, María A De Bortoli, Rocío C Baro Vila, Franco N Ballari, Mirta Diez
{"title":"急性心力衰竭右心室解耦伴射血分数保留或轻度降低:预测长期死亡率的简单参数。","authors":"Lucrecia M Burgos, Lucía Campos Cervera, María A De Bortoli, Rocío C Baro Vila, Franco N Ballari, Mirta Diez","doi":"10.47487/apcyccv.v6i2.466","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Risk prediction in acute heart failure (AHF) has led to the development of multiple prognostic models. Emerging data highlight the prognostic significance of right ventricular (RV) to pulmonary artery (PA) uncoupling, which has been linked to adverse outcomes. Among patients with heart failure with preserved ejection fraction (HFpEF) and mildly reduced ejection fraction (HFmrEF), a highly heterogeneous group, the prognostic relevance of RV-PA uncoupling in forecasting long-term mortality is still not well defined. This study aimed to evaluate the association between RV-PA uncoupling and long-term mortality in a cohort of hospitalized HFpEF and HFmrEF patients.</p><p><strong>Materials and methods: </strong>We performed a retrospective analysis based on a prospective registry of adult patients admitted with a primary diagnosis of AHF between 2015 and 2020. Eligible patients had a left ventricular ejection fraction (LVEF) > 40%. The main outcome was all-cause mortality over long-term follow-up. RV-PA coupling was quantified using the ratio between tricuspid annular plane systolic excursion (TAPSE) and systolic pulmonary artery pressure (sPAP).</p><p><strong>Results: </strong>Out of 465 patients, simultaneous estimation of TAPSE and sPAP was feasible in 361 cases (77%). During a median follow-up of 20.9 months, 100 patients (27.7%) died. A TAPSE/sPAP ratio of 0.38 was identified as the optimal cut-off for risk discrimination. Notably, 41.8% of patients had values below this threshold. Multivariable analysis confirmed that RV-PA uncoupling (TAPSE/sPAP < 0.38) was independently associated with increased long-term mortality (HR: 2.21; 95% CI 1.26-3.81; P = 0.005).</p><p><strong>Conclusion: </strong>In patients hospitalized for AHF with preserved and mildly reduced ejection fraction, RV-PA uncoupling, as determined by the TAPSE/sPAP ratio, was independently associated with long-term all-cause mortality. This echocardiographic parameter may help identify a subgroup of patients at higher risk during follow-up.</p>","PeriodicalId":72295,"journal":{"name":"Archivos Peruanos de cardiologia y cirugia cardiovascular","volume":"6 2","pages":"83-89"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288735/pdf/","citationCount":"0","resultStr":"{\"title\":\"Right ventricular uncoupling in acute heart failure with preserved or mildly reduced ejection fraction: a simple parameter to predict long-term mortality.\",\"authors\":\"Lucrecia M Burgos, Lucía Campos Cervera, María A De Bortoli, Rocío C Baro Vila, Franco N Ballari, Mirta Diez\",\"doi\":\"10.47487/apcyccv.v6i2.466\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Risk prediction in acute heart failure (AHF) has led to the development of multiple prognostic models. Emerging data highlight the prognostic significance of right ventricular (RV) to pulmonary artery (PA) uncoupling, which has been linked to adverse outcomes. Among patients with heart failure with preserved ejection fraction (HFpEF) and mildly reduced ejection fraction (HFmrEF), a highly heterogeneous group, the prognostic relevance of RV-PA uncoupling in forecasting long-term mortality is still not well defined. This study aimed to evaluate the association between RV-PA uncoupling and long-term mortality in a cohort of hospitalized HFpEF and HFmrEF patients.</p><p><strong>Materials and methods: </strong>We performed a retrospective analysis based on a prospective registry of adult patients admitted with a primary diagnosis of AHF between 2015 and 2020. Eligible patients had a left ventricular ejection fraction (LVEF) > 40%. The main outcome was all-cause mortality over long-term follow-up. RV-PA coupling was quantified using the ratio between tricuspid annular plane systolic excursion (TAPSE) and systolic pulmonary artery pressure (sPAP).</p><p><strong>Results: </strong>Out of 465 patients, simultaneous estimation of TAPSE and sPAP was feasible in 361 cases (77%). During a median follow-up of 20.9 months, 100 patients (27.7%) died. A TAPSE/sPAP ratio of 0.38 was identified as the optimal cut-off for risk discrimination. Notably, 41.8% of patients had values below this threshold. Multivariable analysis confirmed that RV-PA uncoupling (TAPSE/sPAP < 0.38) was independently associated with increased long-term mortality (HR: 2.21; 95% CI 1.26-3.81; P = 0.005).</p><p><strong>Conclusion: </strong>In patients hospitalized for AHF with preserved and mildly reduced ejection fraction, RV-PA uncoupling, as determined by the TAPSE/sPAP ratio, was independently associated with long-term all-cause mortality. This echocardiographic parameter may help identify a subgroup of patients at higher risk during follow-up.</p>\",\"PeriodicalId\":72295,\"journal\":{\"name\":\"Archivos Peruanos de cardiologia y cirugia cardiovascular\",\"volume\":\"6 2\",\"pages\":\"83-89\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288735/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archivos Peruanos de cardiologia y cirugia cardiovascular\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.47487/apcyccv.v6i2.466\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archivos Peruanos de cardiologia y cirugia cardiovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.47487/apcyccv.v6i2.466","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
急性心力衰竭(AHF)的风险预测导致了多种预后模型的发展。新出现的数据强调了右心室(RV)与肺动脉(PA)分离的预后意义,这与不良结局有关。在保留射血分数(HFpEF)和轻度降低射血分数(HFmrEF)的心力衰竭患者中,一个高度异质性的群体,RV-PA解耦在预测长期死亡率方面的预后相关性仍然没有很好的定义。本研究旨在评估住院HFpEF和HFmrEF患者的RV-PA解耦与长期死亡率之间的关系。材料和方法:我们对2015年至2020年间初步诊断为AHF的成年患者的前瞻性登记进行了回顾性分析。符合条件的患者左室射血分数(LVEF)为40%。主要结果是长期随访的全因死亡率。利用三尖瓣环形平面收缩偏移(TAPSE)和收缩期肺动脉压(sPAP)之比量化RV-PA耦合。结果:在465例患者中,361例(77%)可以同时估计TAPSE和sPAP。在中位随访20.9个月期间,100名患者(27.7%)死亡。TAPSE/sPAP比值0.38被确定为风险识别的最佳截止值。值得注意的是,41.8%的患者的值低于这个阈值。多变量分析证实,RV-PA解耦(TAPSE/sPAP < 0.38)与长期死亡率增加独立相关(HR: 2.21;95% ci 1.26-3.81;P = 0.005)。结论:在射血分数保留和轻度降低的AHF住院患者中,由TAPSE/sPAP比率确定的RV-PA解耦与长期全因死亡率独立相关。该超声心动图参数可在随访中帮助确定高危患者亚组。
Right ventricular uncoupling in acute heart failure with preserved or mildly reduced ejection fraction: a simple parameter to predict long-term mortality.
Introduction: Risk prediction in acute heart failure (AHF) has led to the development of multiple prognostic models. Emerging data highlight the prognostic significance of right ventricular (RV) to pulmonary artery (PA) uncoupling, which has been linked to adverse outcomes. Among patients with heart failure with preserved ejection fraction (HFpEF) and mildly reduced ejection fraction (HFmrEF), a highly heterogeneous group, the prognostic relevance of RV-PA uncoupling in forecasting long-term mortality is still not well defined. This study aimed to evaluate the association between RV-PA uncoupling and long-term mortality in a cohort of hospitalized HFpEF and HFmrEF patients.
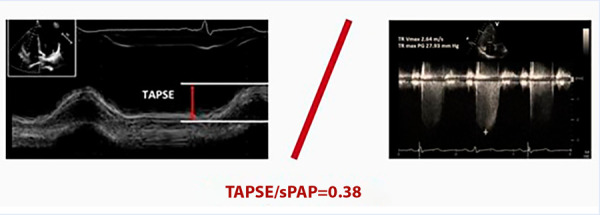
Materials and methods: We performed a retrospective analysis based on a prospective registry of adult patients admitted with a primary diagnosis of AHF between 2015 and 2020. Eligible patients had a left ventricular ejection fraction (LVEF) > 40%. The main outcome was all-cause mortality over long-term follow-up. RV-PA coupling was quantified using the ratio between tricuspid annular plane systolic excursion (TAPSE) and systolic pulmonary artery pressure (sPAP).
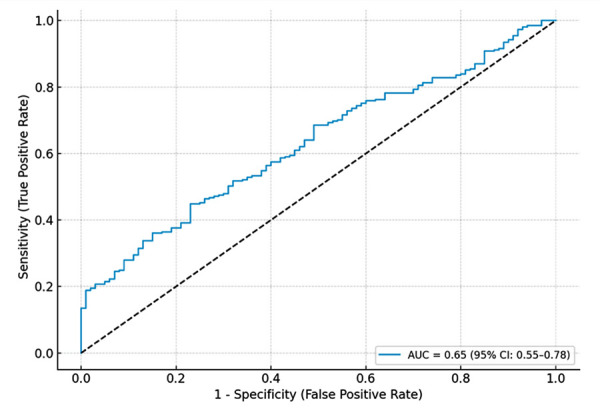
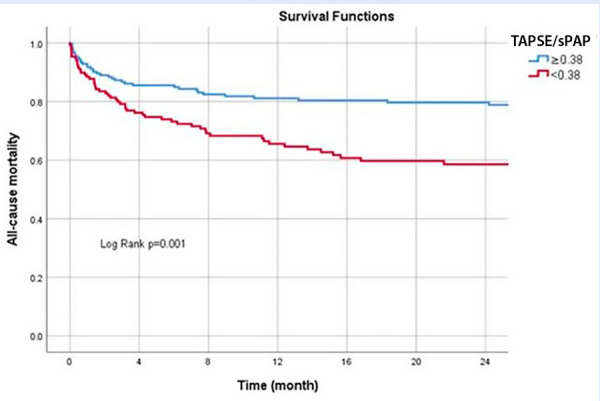
Results: Out of 465 patients, simultaneous estimation of TAPSE and sPAP was feasible in 361 cases (77%). During a median follow-up of 20.9 months, 100 patients (27.7%) died. A TAPSE/sPAP ratio of 0.38 was identified as the optimal cut-off for risk discrimination. Notably, 41.8% of patients had values below this threshold. Multivariable analysis confirmed that RV-PA uncoupling (TAPSE/sPAP < 0.38) was independently associated with increased long-term mortality (HR: 2.21; 95% CI 1.26-3.81; P = 0.005).
Conclusion: In patients hospitalized for AHF with preserved and mildly reduced ejection fraction, RV-PA uncoupling, as determined by the TAPSE/sPAP ratio, was independently associated with long-term all-cause mortality. This echocardiographic parameter may help identify a subgroup of patients at higher risk during follow-up.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


