Zeinab Alnahas, Sujata Sarkar, Kevin T Trowell, Lisa Soltani, Sreekanth Vasireddy
{"title":"抑制Jak在治疗VEXAS中的应用前景,病例报告并文献复习。","authors":"Zeinab Alnahas, Sujata Sarkar, Kevin T Trowell, Lisa Soltani, Sreekanth Vasireddy","doi":"10.2147/OARRR.S531094","DOIUrl":null,"url":null,"abstract":"<p><p>VEXAS syndrome (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) is a recently described adult autoinflammatory disease associated with somatic mutations in the gene encoding ubiquitin-activating enzyme 1 (UBA1) in hematopoietic progenitor cells. Loss of function mutation of UBA1 results in a broad range of inflammatory and hematological conditions. To date, there are no established targeted therapies for VEXAS syndrome, especially in patients who are refractory to conventional immunosuppressive treatments. We report the case of a 75-year-old Hispanic gentleman with hypertension, dyslipidemia, and type 2 diabetes mellitus who presented with a 2-year history of intermittent fever, weight loss, recurrent sore throat, recurrent soft tissue swelling (mimicking cellulitis), oligoarthritis, erythema nodosum, and venous thrombosis. Laboratory workup showed elevated inflammatory markers, macrocytic anemia, and leukopenia. Patient received several rounds of antibiotics and corticosteroids for presumed cellulitis and throat infections, with limited improvement. He subsequently underwent bone marrow biopsy, which showed characteristic vacuolization of myeloid precursors. Genetic testing revealed a missense mutation in UBA1, Exon 3 c.121A>G, pMet41Val. He was diagnosed with VEXAS syndrome. He was started on corticosteroids and Tocilizumab (anti-IL-6 receptor antibody). He had severe leukopenia with Tocilizumab and was switched to Ruxolitinib (Jak inhibitor). He had a significant clinical response to Ruxolitinib and was able to be tapered off prednisone. Our case report and review of the literature report Jak inhibition as a possible target for the management of inflammatory symptoms of VEXAS.</p>","PeriodicalId":45545,"journal":{"name":"Open Access Rheumatology-Research and Reviews","volume":"17 ","pages":"147-156"},"PeriodicalIF":1.7000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12297003/pdf/","citationCount":"0","resultStr":"{\"title\":\"Promise of Jak Inhibition in the Management of VEXAS, Case Report with Review of the Literature.\",\"authors\":\"Zeinab Alnahas, Sujata Sarkar, Kevin T Trowell, Lisa Soltani, Sreekanth Vasireddy\",\"doi\":\"10.2147/OARRR.S531094\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>VEXAS syndrome (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) is a recently described adult autoinflammatory disease associated with somatic mutations in the gene encoding ubiquitin-activating enzyme 1 (UBA1) in hematopoietic progenitor cells. Loss of function mutation of UBA1 results in a broad range of inflammatory and hematological conditions. To date, there are no established targeted therapies for VEXAS syndrome, especially in patients who are refractory to conventional immunosuppressive treatments. We report the case of a 75-year-old Hispanic gentleman with hypertension, dyslipidemia, and type 2 diabetes mellitus who presented with a 2-year history of intermittent fever, weight loss, recurrent sore throat, recurrent soft tissue swelling (mimicking cellulitis), oligoarthritis, erythema nodosum, and venous thrombosis. Laboratory workup showed elevated inflammatory markers, macrocytic anemia, and leukopenia. Patient received several rounds of antibiotics and corticosteroids for presumed cellulitis and throat infections, with limited improvement. He subsequently underwent bone marrow biopsy, which showed characteristic vacuolization of myeloid precursors. Genetic testing revealed a missense mutation in UBA1, Exon 3 c.121A>G, pMet41Val. He was diagnosed with VEXAS syndrome. He was started on corticosteroids and Tocilizumab (anti-IL-6 receptor antibody). He had severe leukopenia with Tocilizumab and was switched to Ruxolitinib (Jak inhibitor). He had a significant clinical response to Ruxolitinib and was able to be tapered off prednisone. Our case report and review of the literature report Jak inhibition as a possible target for the management of inflammatory symptoms of VEXAS.</p>\",\"PeriodicalId\":45545,\"journal\":{\"name\":\"Open Access Rheumatology-Research and Reviews\",\"volume\":\"17 \",\"pages\":\"147-156\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-07-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12297003/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Rheumatology-Research and Reviews\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OARRR.S531094\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Rheumatology-Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OARRR.S531094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Promise of Jak Inhibition in the Management of VEXAS, Case Report with Review of the Literature.
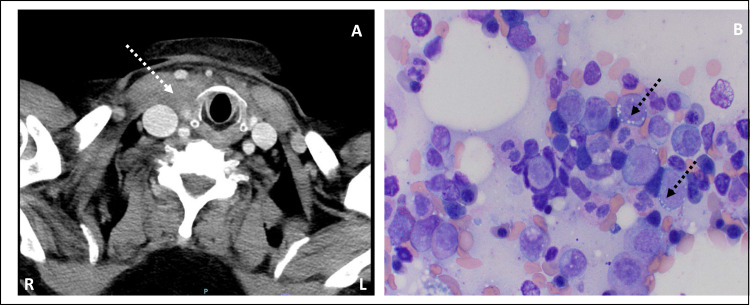
VEXAS syndrome (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) is a recently described adult autoinflammatory disease associated with somatic mutations in the gene encoding ubiquitin-activating enzyme 1 (UBA1) in hematopoietic progenitor cells. Loss of function mutation of UBA1 results in a broad range of inflammatory and hematological conditions. To date, there are no established targeted therapies for VEXAS syndrome, especially in patients who are refractory to conventional immunosuppressive treatments. We report the case of a 75-year-old Hispanic gentleman with hypertension, dyslipidemia, and type 2 diabetes mellitus who presented with a 2-year history of intermittent fever, weight loss, recurrent sore throat, recurrent soft tissue swelling (mimicking cellulitis), oligoarthritis, erythema nodosum, and venous thrombosis. Laboratory workup showed elevated inflammatory markers, macrocytic anemia, and leukopenia. Patient received several rounds of antibiotics and corticosteroids for presumed cellulitis and throat infections, with limited improvement. He subsequently underwent bone marrow biopsy, which showed characteristic vacuolization of myeloid precursors. Genetic testing revealed a missense mutation in UBA1, Exon 3 c.121A>G, pMet41Val. He was diagnosed with VEXAS syndrome. He was started on corticosteroids and Tocilizumab (anti-IL-6 receptor antibody). He had severe leukopenia with Tocilizumab and was switched to Ruxolitinib (Jak inhibitor). He had a significant clinical response to Ruxolitinib and was able to be tapered off prednisone. Our case report and review of the literature report Jak inhibition as a possible target for the management of inflammatory symptoms of VEXAS.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


