Nele Van De Winkel, Ewout Muylle, Emilio Canovai, Irum Amin, Andrew Butler, Rodrigo Vianna, Gennaro Selvaggi, Pablo Farinelli, Gabriel Gondolesi, Carmelo Loinaz, Iago Justo, Hector Vilca-Melendez, Ulrika Skogsberg Dahlgren, Gustaf Herlenius, Alireza Shamsaeefar, Hamed Nikoupour, Antoine Dubois, Marc Miserez, André D'Hoore, Robert Venick, Jacques Pirenne, Laurens J Ceulemans
{"title":"实体器官移植中无血管化直肌筋膜移植的长期结果:一项全球多中心IIRTA调查。","authors":"Nele Van De Winkel, Ewout Muylle, Emilio Canovai, Irum Amin, Andrew Butler, Rodrigo Vianna, Gennaro Selvaggi, Pablo Farinelli, Gabriel Gondolesi, Carmelo Loinaz, Iago Justo, Hector Vilca-Melendez, Ulrika Skogsberg Dahlgren, Gustaf Herlenius, Alireza Shamsaeefar, Hamed Nikoupour, Antoine Dubois, Marc Miserez, André D'Hoore, Robert Venick, Jacques Pirenne, Laurens J Ceulemans","doi":"10.1097/TXD.0000000000001839","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Abdominal wall (AW) closure after solid organ transplantation (SOT) is challenging in case of loss of abdominal domain and/or large-for-size grafts. Primary closure is crucial to avoid open abdomen-associated morbidity and mortality. Several techniques have been developed to address this challenge, including nonvascularized rectus fascia transplantation (NVRF Tx). Long-term outcome is missing.</p><p><strong>Methods: </strong>We designed a multicenter survey to analyze the worldwide experience after NVRF Tx. International Intestinal Rehabilitation And Transplantation Association members were invited to participate to a questionnaire. The survey included all NVRF Tx performed after SOT. Questions were classified into pre-, intra-, and postoperative data.</p><p><strong>Results: </strong>Of the 29 responding centers, 8 performed NVRF Tx, comprising 98 patients in total. Thirty-two patients underwent multivisceral Tx (33.3%), 27 isolated intestinal Tx (28.1%), 21 combined liver-intestinal Tx (21.9%), 8 liver Tx (8.3%), 8 other SOT (8.3%), and 2 (2.0%) not reported. Thirty NVRF (30.9%) were from third-party donors. Thirty patients (31.3%) had surgical site infections. Seventy-one (74.0%) patients had reoperations, of them 18 (26.1%) patients had NVRF removal. Median follow-up time was 31 mo (10.0-63.5). Seventeen patients presented with bulging of the AW (18.7%), 5 with herniation (5.9%). No NVRF graft rejection was reported.</p><p><strong>Conclusions: </strong>This survey reports long-term outcome after NVRF Tx, with herniation in a limited number of patients, no suspicion of clinical rejection and no additional infection and mortality. NVRF Tx has proven to be a useful option, belonging to the standard armamentarium for AW closure after SOT.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"11 8","pages":"e1839"},"PeriodicalIF":1.9000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12289136/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term Outcome After Nonvascularized Rectus Fascia Transplantation in Solid Organ Transplantation: A Global Multicenter IIRTA Survey.\",\"authors\":\"Nele Van De Winkel, Ewout Muylle, Emilio Canovai, Irum Amin, Andrew Butler, Rodrigo Vianna, Gennaro Selvaggi, Pablo Farinelli, Gabriel Gondolesi, Carmelo Loinaz, Iago Justo, Hector Vilca-Melendez, Ulrika Skogsberg Dahlgren, Gustaf Herlenius, Alireza Shamsaeefar, Hamed Nikoupour, Antoine Dubois, Marc Miserez, André D'Hoore, Robert Venick, Jacques Pirenne, Laurens J Ceulemans\",\"doi\":\"10.1097/TXD.0000000000001839\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Abdominal wall (AW) closure after solid organ transplantation (SOT) is challenging in case of loss of abdominal domain and/or large-for-size grafts. Primary closure is crucial to avoid open abdomen-associated morbidity and mortality. Several techniques have been developed to address this challenge, including nonvascularized rectus fascia transplantation (NVRF Tx). Long-term outcome is missing.</p><p><strong>Methods: </strong>We designed a multicenter survey to analyze the worldwide experience after NVRF Tx. International Intestinal Rehabilitation And Transplantation Association members were invited to participate to a questionnaire. The survey included all NVRF Tx performed after SOT. Questions were classified into pre-, intra-, and postoperative data.</p><p><strong>Results: </strong>Of the 29 responding centers, 8 performed NVRF Tx, comprising 98 patients in total. Thirty-two patients underwent multivisceral Tx (33.3%), 27 isolated intestinal Tx (28.1%), 21 combined liver-intestinal Tx (21.9%), 8 liver Tx (8.3%), 8 other SOT (8.3%), and 2 (2.0%) not reported. Thirty NVRF (30.9%) were from third-party donors. Thirty patients (31.3%) had surgical site infections. Seventy-one (74.0%) patients had reoperations, of them 18 (26.1%) patients had NVRF removal. Median follow-up time was 31 mo (10.0-63.5). Seventeen patients presented with bulging of the AW (18.7%), 5 with herniation (5.9%). No NVRF graft rejection was reported.</p><p><strong>Conclusions: </strong>This survey reports long-term outcome after NVRF Tx, with herniation in a limited number of patients, no suspicion of clinical rejection and no additional infection and mortality. NVRF Tx has proven to be a useful option, belonging to the standard armamentarium for AW closure after SOT.</p>\",\"PeriodicalId\":23225,\"journal\":{\"name\":\"Transplantation Direct\",\"volume\":\"11 8\",\"pages\":\"e1839\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12289136/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplantation Direct\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/TXD.0000000000001839\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001839","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
Long-term Outcome After Nonvascularized Rectus Fascia Transplantation in Solid Organ Transplantation: A Global Multicenter IIRTA Survey.
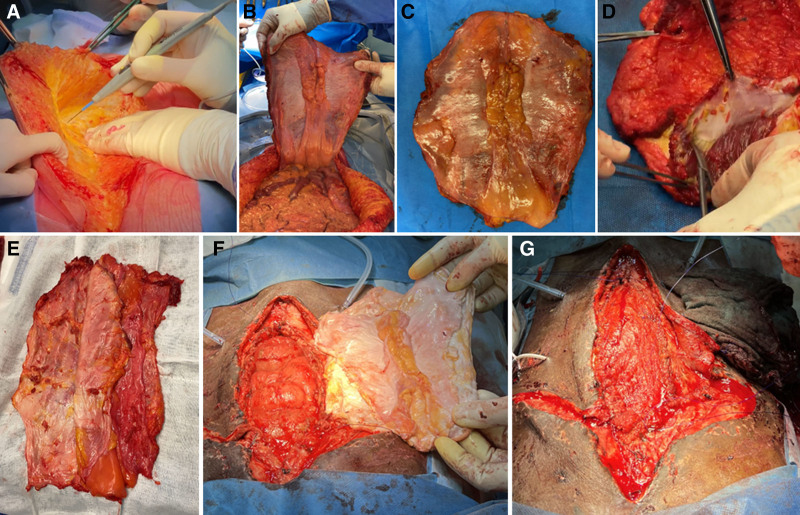
Background: Abdominal wall (AW) closure after solid organ transplantation (SOT) is challenging in case of loss of abdominal domain and/or large-for-size grafts. Primary closure is crucial to avoid open abdomen-associated morbidity and mortality. Several techniques have been developed to address this challenge, including nonvascularized rectus fascia transplantation (NVRF Tx). Long-term outcome is missing.
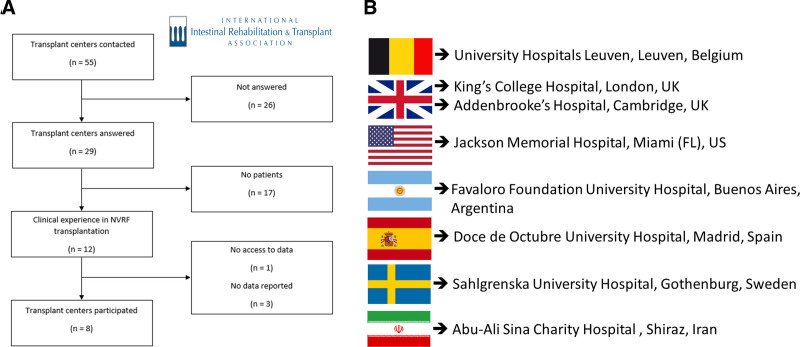
Methods: We designed a multicenter survey to analyze the worldwide experience after NVRF Tx. International Intestinal Rehabilitation And Transplantation Association members were invited to participate to a questionnaire. The survey included all NVRF Tx performed after SOT. Questions were classified into pre-, intra-, and postoperative data.
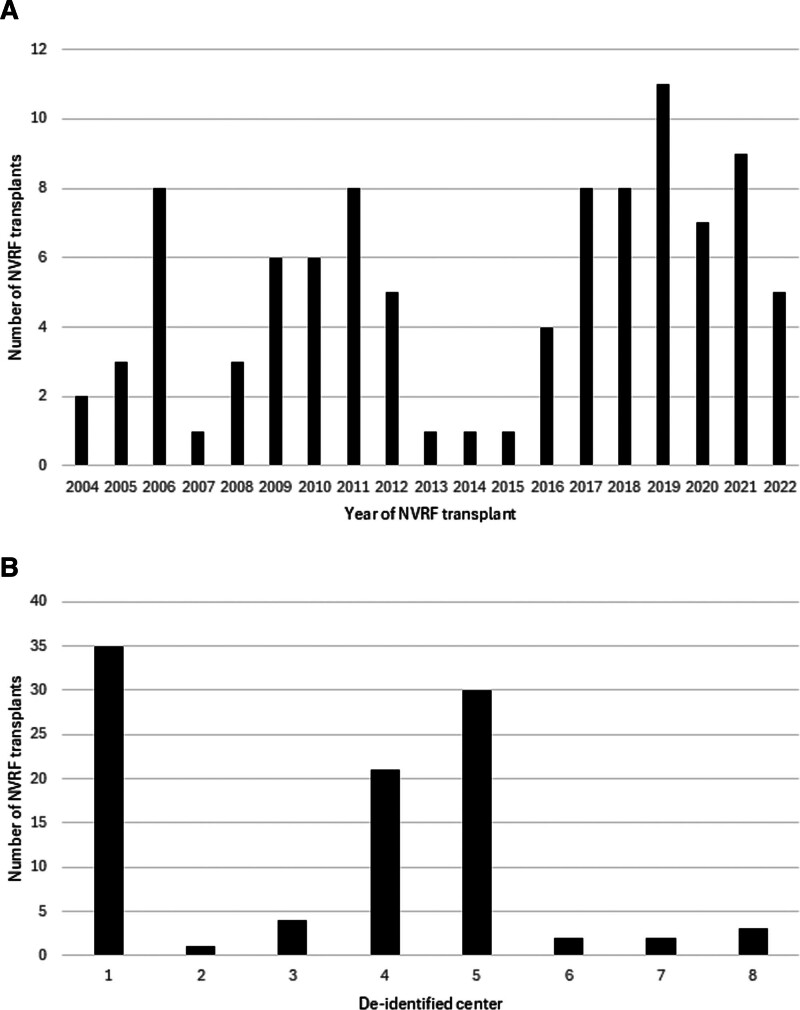
Results: Of the 29 responding centers, 8 performed NVRF Tx, comprising 98 patients in total. Thirty-two patients underwent multivisceral Tx (33.3%), 27 isolated intestinal Tx (28.1%), 21 combined liver-intestinal Tx (21.9%), 8 liver Tx (8.3%), 8 other SOT (8.3%), and 2 (2.0%) not reported. Thirty NVRF (30.9%) were from third-party donors. Thirty patients (31.3%) had surgical site infections. Seventy-one (74.0%) patients had reoperations, of them 18 (26.1%) patients had NVRF removal. Median follow-up time was 31 mo (10.0-63.5). Seventeen patients presented with bulging of the AW (18.7%), 5 with herniation (5.9%). No NVRF graft rejection was reported.
Conclusions: This survey reports long-term outcome after NVRF Tx, with herniation in a limited number of patients, no suspicion of clinical rejection and no additional infection and mortality. NVRF Tx has proven to be a useful option, belonging to the standard armamentarium for AW closure after SOT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


