Su Yeon Lee, Jin Won Huh, Sang-Bum Hong, Chae-Man Lim, Jee Hwan Ahn
{"title":"一项回顾性队列研究表明,ICU出院时的身体和认知障碍与患有实体恶性肿瘤的ICU幸存者的高长期死亡率相关。","authors":"Su Yeon Lee, Jin Won Huh, Sang-Bum Hong, Chae-Man Lim, Jee Hwan Ahn","doi":"10.2147/TCRM.S520206","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Many ICU survivors experience post-ICU physical, cognitive, or mental impairments. In ICU survivors with solid malignancies, post-ICU impairments can impede further cancer treatments and negatively impact their outcomes. This study aimed to investigate post-ICU mortalities and their risk factors at ICU discharge in ICU survivors with solid malignancies.</p><p><strong>Methods: </strong>In this retrospective cohort study, adult patients with solid malignancies who were unexpectedly admitted to the medical ICU of a tertiary hospital between 2016 and 2022 and survived to ICU discharge were included. Data at ICU discharge were collected from electronic medical records. In-hospital and 1-year mortality and their risk factors were analyzed.</p><p><strong>Results: </strong>Of the 708 ICU survivors, 25.1% died in the hospital, and 61% died within one year. At ICU discharge, 20.9% had delirium, 3.8% had coma, and 80.6% had impaired mobility. Respiratory support, including bilevel positive airway pressure (BiPAP), high-flow nasal cannula (HFNC), or other oxygen therapies was used in 88.7% of patients. Delirium (adjusted OR 1.73; 95% CI 1.04-2.87; p = 0.035), coma (adjusted OR 5.63; 95% CI 2.09-16.17; p < 0.001), limited mobility (adjusted OR 2.41; 95% CI 1.22-5.14; p = 0.015), and use of BiPAP (adjusted OR 21.63; 95% CI 5.36-99.57; p < 0.001) or HFNC (adjusted OR 7.08; 95% CI 2.45-23.99; p < 0.001) were independently associated with in-hospital mortality. One-year survival was significantly lower in patients with delirium (35%, p < 0.001), coma (26%, p < 0.001), limited mobility (37%, p = 0.003), or those receiving respiratory support at ICU discharge (35%, p < 0.001).</p><p><strong>Conclusion: </strong>A considerable portion of ICU survivors with solid malignancies died in the hospital or within one year after ICU discharge in our study. Cognitive, mobility, and pulmonary impairments at ICU discharge were significant risk factors for both in-hospital and long-term mortality.</p>","PeriodicalId":22977,"journal":{"name":"Therapeutics and Clinical Risk Management","volume":"21 ","pages":"1121-1133"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12296672/pdf/","citationCount":"0","resultStr":"{\"title\":\"Physical and Cognitive Impairments at ICU Discharge are Associated with High Long-Term Mortality in ICU Survivors with Solid Malignancies: A Retrospective Cohort Study.\",\"authors\":\"Su Yeon Lee, Jin Won Huh, Sang-Bum Hong, Chae-Man Lim, Jee Hwan Ahn\",\"doi\":\"10.2147/TCRM.S520206\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Many ICU survivors experience post-ICU physical, cognitive, or mental impairments. In ICU survivors with solid malignancies, post-ICU impairments can impede further cancer treatments and negatively impact their outcomes. This study aimed to investigate post-ICU mortalities and their risk factors at ICU discharge in ICU survivors with solid malignancies.</p><p><strong>Methods: </strong>In this retrospective cohort study, adult patients with solid malignancies who were unexpectedly admitted to the medical ICU of a tertiary hospital between 2016 and 2022 and survived to ICU discharge were included. Data at ICU discharge were collected from electronic medical records. In-hospital and 1-year mortality and their risk factors were analyzed.</p><p><strong>Results: </strong>Of the 708 ICU survivors, 25.1% died in the hospital, and 61% died within one year. At ICU discharge, 20.9% had delirium, 3.8% had coma, and 80.6% had impaired mobility. Respiratory support, including bilevel positive airway pressure (BiPAP), high-flow nasal cannula (HFNC), or other oxygen therapies was used in 88.7% of patients. Delirium (adjusted OR 1.73; 95% CI 1.04-2.87; p = 0.035), coma (adjusted OR 5.63; 95% CI 2.09-16.17; p < 0.001), limited mobility (adjusted OR 2.41; 95% CI 1.22-5.14; p = 0.015), and use of BiPAP (adjusted OR 21.63; 95% CI 5.36-99.57; p < 0.001) or HFNC (adjusted OR 7.08; 95% CI 2.45-23.99; p < 0.001) were independently associated with in-hospital mortality. One-year survival was significantly lower in patients with delirium (35%, p < 0.001), coma (26%, p < 0.001), limited mobility (37%, p = 0.003), or those receiving respiratory support at ICU discharge (35%, p < 0.001).</p><p><strong>Conclusion: </strong>A considerable portion of ICU survivors with solid malignancies died in the hospital or within one year after ICU discharge in our study. Cognitive, mobility, and pulmonary impairments at ICU discharge were significant risk factors for both in-hospital and long-term mortality.</p>\",\"PeriodicalId\":22977,\"journal\":{\"name\":\"Therapeutics and Clinical Risk Management\",\"volume\":\"21 \",\"pages\":\"1121-1133\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-07-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12296672/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutics and Clinical Risk Management\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/TCRM.S520206\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"Pharmacology, Toxicology and Pharmaceutics\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutics and Clinical Risk Management","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/TCRM.S520206","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Pharmacology, Toxicology and Pharmaceutics","Score":null,"Total":0}
引用次数: 0
摘要
背景:许多ICU幸存者经历了ICU后的身体、认知或精神损伤。在患有实体恶性肿瘤的ICU幸存者中,ICU后的损伤可能阻碍进一步的癌症治疗并对其结果产生负面影响。本研究旨在探讨实性恶性肿瘤ICU幸存者出院时ICU后死亡率及其危险因素。方法:本回顾性队列研究纳入2016 - 2022年间意外入住某三级医院内科ICU并存活至ICU出院的成年实体恶性肿瘤患者。ICU出院时的数据从电子病历中收集。分析住院死亡率和1年死亡率及其危险因素。结果:708例ICU存活患者中,25.1%在医院死亡,61%在1年内死亡。出院时,20.9%出现谵妄,3.8%出现昏迷,80.6%出现活动能力受损。88.7%的患者使用呼吸支持,包括双水平气道正压通气(BiPAP)、高流量鼻插管(HFNC)或其他氧疗。谵妄(调整OR 1.73;95% ci 1.04-2.87;p = 0.035),昏迷(调整OR 5.63;95% ci 2.09-16.17;p < 0.001),活动受限(调整OR为2.41;95% ci 1.22-5.14;p = 0.015), BiPAP的使用(调整OR为21.63;95% ci 5.36-99.57;p < 0.001)或HFNC(调整or为7.08;95% ci 2.45-23.99;P < 0.001)与住院死亡率独立相关。谵妄(35%,p < 0.001)、昏迷(26%,p < 0.001)、活动受限(37%,p = 0.003)或ICU出院时接受呼吸支持(35%,p < 0.001)患者的1年生存率显著降低。结论:在我们的研究中,有相当一部分患有实体恶性肿瘤的ICU幸存者在医院或出院后一年内死亡。ICU出院时的认知、活动能力和肺部损伤是住院死亡率和长期死亡率的重要危险因素。
Physical and Cognitive Impairments at ICU Discharge are Associated with High Long-Term Mortality in ICU Survivors with Solid Malignancies: A Retrospective Cohort Study.
Background: Many ICU survivors experience post-ICU physical, cognitive, or mental impairments. In ICU survivors with solid malignancies, post-ICU impairments can impede further cancer treatments and negatively impact their outcomes. This study aimed to investigate post-ICU mortalities and their risk factors at ICU discharge in ICU survivors with solid malignancies.
Methods: In this retrospective cohort study, adult patients with solid malignancies who were unexpectedly admitted to the medical ICU of a tertiary hospital between 2016 and 2022 and survived to ICU discharge were included. Data at ICU discharge were collected from electronic medical records. In-hospital and 1-year mortality and their risk factors were analyzed.
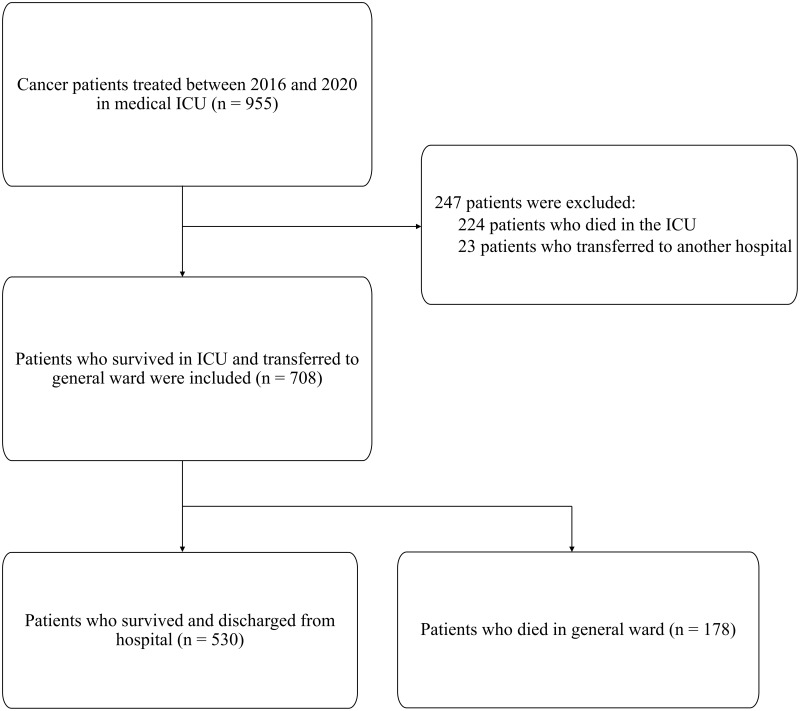
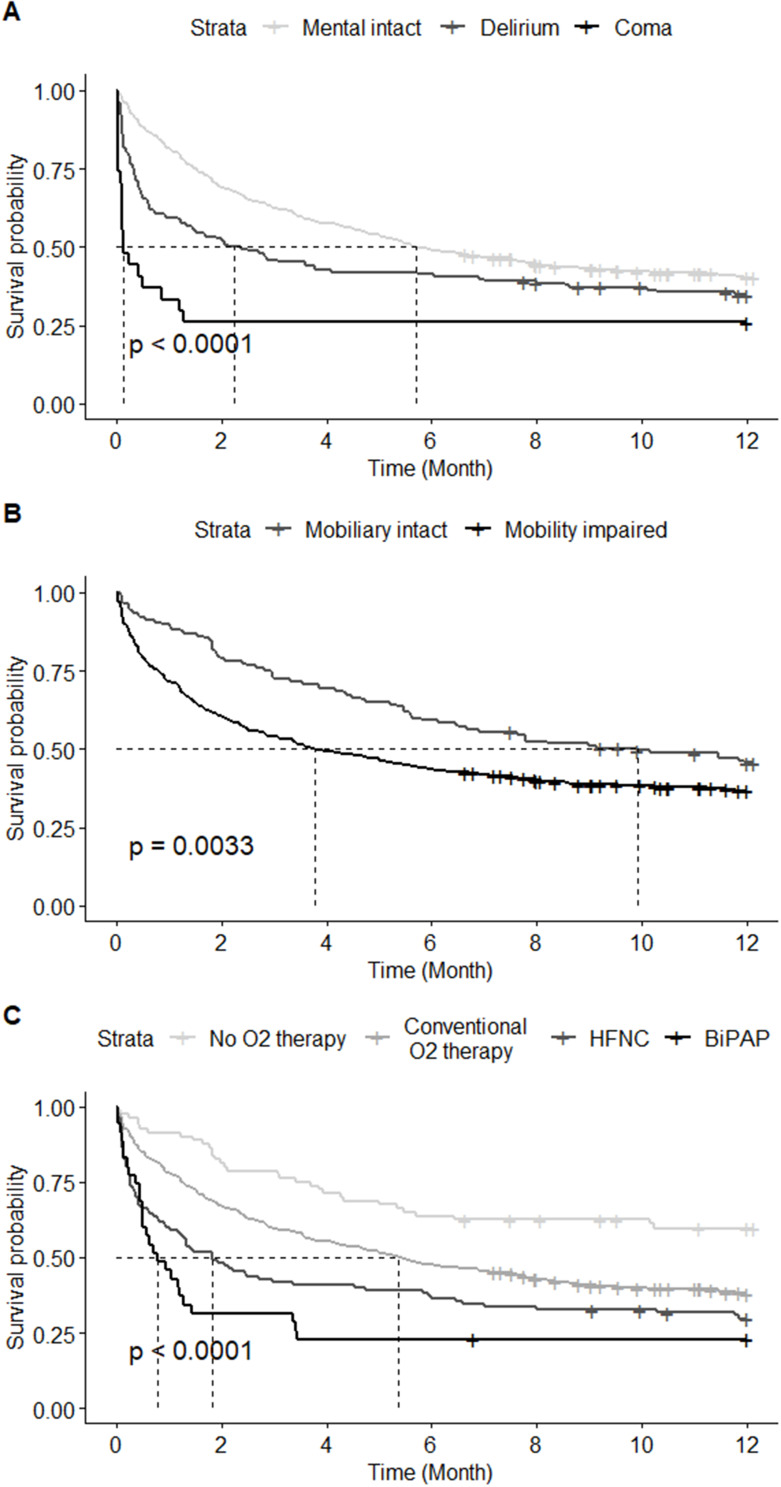
Results: Of the 708 ICU survivors, 25.1% died in the hospital, and 61% died within one year. At ICU discharge, 20.9% had delirium, 3.8% had coma, and 80.6% had impaired mobility. Respiratory support, including bilevel positive airway pressure (BiPAP), high-flow nasal cannula (HFNC), or other oxygen therapies was used in 88.7% of patients. Delirium (adjusted OR 1.73; 95% CI 1.04-2.87; p = 0.035), coma (adjusted OR 5.63; 95% CI 2.09-16.17; p < 0.001), limited mobility (adjusted OR 2.41; 95% CI 1.22-5.14; p = 0.015), and use of BiPAP (adjusted OR 21.63; 95% CI 5.36-99.57; p < 0.001) or HFNC (adjusted OR 7.08; 95% CI 2.45-23.99; p < 0.001) were independently associated with in-hospital mortality. One-year survival was significantly lower in patients with delirium (35%, p < 0.001), coma (26%, p < 0.001), limited mobility (37%, p = 0.003), or those receiving respiratory support at ICU discharge (35%, p < 0.001).
Conclusion: A considerable portion of ICU survivors with solid malignancies died in the hospital or within one year after ICU discharge in our study. Cognitive, mobility, and pulmonary impairments at ICU discharge were significant risk factors for both in-hospital and long-term mortality.
期刊介绍:
Therapeutics and Clinical Risk Management is an international, peer-reviewed journal of clinical therapeutics and risk management, focusing on concise rapid reporting of clinical studies in all therapeutic areas, outcomes, safety, and programs for the effective, safe, and sustained use of medicines, therapeutic and surgical interventions in all clinical areas.
The journal welcomes submissions covering original research, clinical and epidemiological studies, reviews, guidelines, expert opinion and commentary. The journal will consider case reports but only if they make a valuable and original contribution to the literature.
As of 18th March 2019, Therapeutics and Clinical Risk Management will no longer consider meta-analyses for publication.
The journal does not accept study protocols, animal-based or cell line-based studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


