Tonje R Johannessen, Indra M B Melessen, Odd Martin Vallersnes, Amy Manten, Sigrun Halvorsen, Dan Atar, Ralf E Harskamp
{"title":"在急诊初级护理中充分识别低风险胸痛:基于两个欧洲队列评估preHEAR(T)的表现","authors":"Tonje R Johannessen, Indra M B Melessen, Odd Martin Vallersnes, Amy Manten, Sigrun Halvorsen, Dan Atar, Ralf E Harskamp","doi":"10.1136/openhrt-2025-003362","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Differentiating cardiac from non-cardiac acute chest pain poses a diagnostic challenge, especially in primary care. The History, ECG, Age, Risk factors and Troponin level (HEART) score aid in risk stratification in hospitals, while the prehospital HEART (preHEART) score was refined for paramedics' use. However, its accuracy in emergency primary care has not been studied. This study evaluates the preHEAR(T) score, with and without high-sensitivity cardiac troponin (hs-cTn), as a tool to rule out acute myocardial infarction (MI) in emergency primary care.</p><p><strong>Methods: </strong>Retrospective data from two European cohorts were analysed, namely the One-hoUr Troponin in a low-prevalence population of Acute Coronary Syndrome (OUT-ACS) study (1711 patients) at a Norwegian emergency primary care centre (2016-2018) and the TRiage of Acute Chest pain Evaluated in urgent primary care (TRACE) study (664 patients) at a Dutch emergency primary care centre (2017). The preHEAR (without hs-cTn) score was evaluated in both cohorts. The preHEART score was assessed in OUT-ACS only, as the TRACE study did not measure troponins. The threshold of ≤3 points has previously been determined as low risk for acute MI (AMI) and optimal for rule-out purposes. The primary outcome was diagnostic performance for ruling out MI, and the secondary outcome was the composite of 90-day AMI or all-cause death.</p><p><strong>Results: </strong>In OUT-ACS, 3.6% of patients had an AMI (median age 56 years (45-68); 47.7% female), and 3% in TRACE (median age 48 years (32-67); 56.9% female). PreHEAR identified 49.3% (OUT-ACS) and 82.7% (TRACE) as low risk, while preHEART identified 33.6% (OUT-ACS) as low risk. Sensitivity/specificity for AMI were 63.9% (95% CI 50.6 to 75.8)/49.8% (95% CI 47.3 to 52.7) (OUT-ACS) and 65% (95% CI 40.8 to 84.6)/84.2% (95% CI 81.1 to 86.9) (TRACE) for preHEAR and 93.4% (95% CI 84.1 to 98.2)/34.6% (95% CI 32.2 to 37) for preHEART. For the secondary outcome, similar diagnostic performance metrics were found. There were four missed AMI cases in the low-risk preHEART group, who were all female.</p><p><strong>Conclusion: </strong>Neither the preHEAR nor preHEART scores provide sufficient rule out safety in emergency primary care and may particularly underestimate AMI risk in females.</p><p><strong>Trial registration number: </strong>OUT-ACS: clinicaltrials.gov NCT02983123.</p><p><strong>Trace: </strong>Netherlands Trial Registry (NL-OMON20102); https://onderzoekmetmensen.nl/nl/trial/20102.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 2","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12306204/pdf/","citationCount":"0","resultStr":"{\"title\":\"Adequately identifying low-risk chest pain in emergency primary care: evaluating the performance of preHEAR(T) based on two European cohorts.\",\"authors\":\"Tonje R Johannessen, Indra M B Melessen, Odd Martin Vallersnes, Amy Manten, Sigrun Halvorsen, Dan Atar, Ralf E Harskamp\",\"doi\":\"10.1136/openhrt-2025-003362\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Differentiating cardiac from non-cardiac acute chest pain poses a diagnostic challenge, especially in primary care. The History, ECG, Age, Risk factors and Troponin level (HEART) score aid in risk stratification in hospitals, while the prehospital HEART (preHEART) score was refined for paramedics' use. However, its accuracy in emergency primary care has not been studied. This study evaluates the preHEAR(T) score, with and without high-sensitivity cardiac troponin (hs-cTn), as a tool to rule out acute myocardial infarction (MI) in emergency primary care.</p><p><strong>Methods: </strong>Retrospective data from two European cohorts were analysed, namely the One-hoUr Troponin in a low-prevalence population of Acute Coronary Syndrome (OUT-ACS) study (1711 patients) at a Norwegian emergency primary care centre (2016-2018) and the TRiage of Acute Chest pain Evaluated in urgent primary care (TRACE) study (664 patients) at a Dutch emergency primary care centre (2017). The preHEAR (without hs-cTn) score was evaluated in both cohorts. The preHEART score was assessed in OUT-ACS only, as the TRACE study did not measure troponins. The threshold of ≤3 points has previously been determined as low risk for acute MI (AMI) and optimal for rule-out purposes. The primary outcome was diagnostic performance for ruling out MI, and the secondary outcome was the composite of 90-day AMI or all-cause death.</p><p><strong>Results: </strong>In OUT-ACS, 3.6% of patients had an AMI (median age 56 years (45-68); 47.7% female), and 3% in TRACE (median age 48 years (32-67); 56.9% female). PreHEAR identified 49.3% (OUT-ACS) and 82.7% (TRACE) as low risk, while preHEART identified 33.6% (OUT-ACS) as low risk. Sensitivity/specificity for AMI were 63.9% (95% CI 50.6 to 75.8)/49.8% (95% CI 47.3 to 52.7) (OUT-ACS) and 65% (95% CI 40.8 to 84.6)/84.2% (95% CI 81.1 to 86.9) (TRACE) for preHEAR and 93.4% (95% CI 84.1 to 98.2)/34.6% (95% CI 32.2 to 37) for preHEART. For the secondary outcome, similar diagnostic performance metrics were found. There were four missed AMI cases in the low-risk preHEART group, who were all female.</p><p><strong>Conclusion: </strong>Neither the preHEAR nor preHEART scores provide sufficient rule out safety in emergency primary care and may particularly underestimate AMI risk in females.</p><p><strong>Trial registration number: </strong>OUT-ACS: clinicaltrials.gov NCT02983123.</p><p><strong>Trace: </strong>Netherlands Trial Registry (NL-OMON20102); https://onderzoekmetmensen.nl/nl/trial/20102.</p>\",\"PeriodicalId\":19505,\"journal\":{\"name\":\"Open Heart\",\"volume\":\"12 2\",\"pages\":\"\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12306204/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/openhrt-2025-003362\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003362","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:鉴别心源性与非心源性急性胸痛是一项诊断挑战,特别是在初级保健中。病史、心电图、年龄、危险因素和肌钙蛋白水平(HEART)评分有助于医院的风险分层,而院前心脏(preHEART)评分则被改进以供护理人员使用。然而,其在急诊初级保健中的准确性尚未得到研究。本研究评估了有和没有高敏感性心肌肌钙蛋白(hs-cTn)的preHEAR(T)评分,作为在急诊初级保健中排除急性心肌梗死(MI)的工具。方法:分析了来自两个欧洲队列的回顾性数据,即挪威紧急初级保健中心(2016-2018年)的低患病率急性冠状动脉综合征人群(OUT-ACS)研究(1711例患者)和荷兰紧急初级保健中心(2017年)的急性胸痛分诊评估(TRACE)研究(664例患者)。在两个队列中评估preHEAR(不含hs-cTn)评分。由于TRACE研究没有测量肌钙蛋白,因此仅在OUT-ACS中评估了preHEART评分。阈值≤3分以前被确定为急性心肌梗死(AMI)的低风险,并且是最佳的排除目的。主要终点是排除心肌梗死的诊断表现,次要终点是90天内心肌梗死或全因死亡的综合结果。结果:在OUT-ACS中,3.6%的患者发生AMI(中位年龄56岁(45-68岁);女性47.7%),TRACE组为3%(中位年龄48岁(32-67岁);56.9%的女性)。PreHEAR鉴定49.3% (OUT-ACS)和82.7% (TRACE)为低风险,而preHEART鉴定33.6% (OUT-ACS)为低风险。AMI的敏感性/特异性为63.9% (95% CI 50.6 ~ 75.8)/49.8% (95% CI 47.3 ~ 52.7) (OUT-ACS), preHEAR的敏感性/特异性为65% (95% CI 40.8 ~ 84.6)/84.2% (95% CI 81.1 ~ 86.9) (TRACE), preHEART的敏感性/特异性为93.4% (95% CI 84.1 ~ 98.2)/34.6% (95% CI 32.2 ~ 37)。对于次要结局,发现了类似的诊断性能指标。低危pre - heart组有4例AMI漏诊,均为女性。结论:无论是preHEAR还是preHEART评分都不能充分排除急诊初级保健的安全性,尤其可能低估了女性AMI的风险。试验注册号:OUT-ACS: clinicaltrials.gov NCT02983123。追踪:荷兰试验登记处(NL-OMON20102);https://onderzoekmetmensen.nl/nl/trial/20102。
Adequately identifying low-risk chest pain in emergency primary care: evaluating the performance of preHEAR(T) based on two European cohorts.
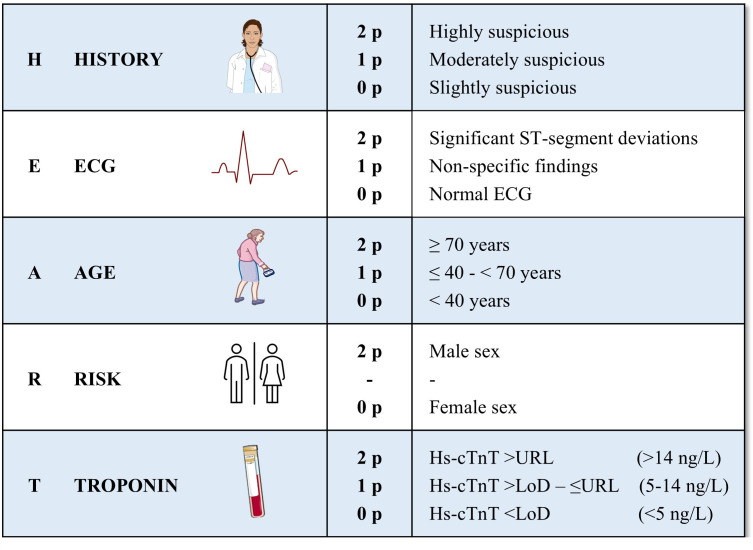
Background: Differentiating cardiac from non-cardiac acute chest pain poses a diagnostic challenge, especially in primary care. The History, ECG, Age, Risk factors and Troponin level (HEART) score aid in risk stratification in hospitals, while the prehospital HEART (preHEART) score was refined for paramedics' use. However, its accuracy in emergency primary care has not been studied. This study evaluates the preHEAR(T) score, with and without high-sensitivity cardiac troponin (hs-cTn), as a tool to rule out acute myocardial infarction (MI) in emergency primary care.
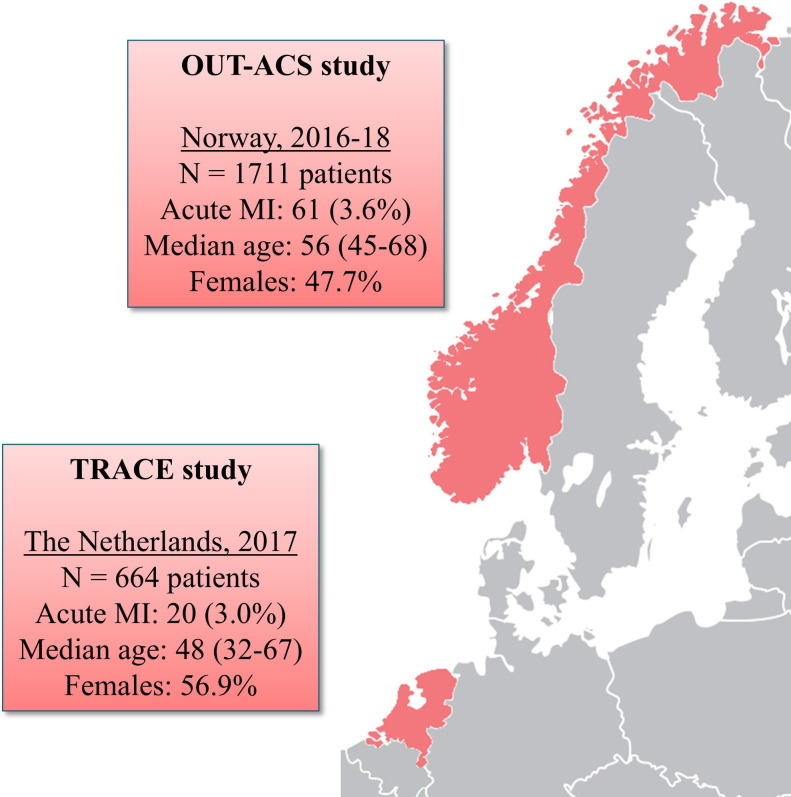
Methods: Retrospective data from two European cohorts were analysed, namely the One-hoUr Troponin in a low-prevalence population of Acute Coronary Syndrome (OUT-ACS) study (1711 patients) at a Norwegian emergency primary care centre (2016-2018) and the TRiage of Acute Chest pain Evaluated in urgent primary care (TRACE) study (664 patients) at a Dutch emergency primary care centre (2017). The preHEAR (without hs-cTn) score was evaluated in both cohorts. The preHEART score was assessed in OUT-ACS only, as the TRACE study did not measure troponins. The threshold of ≤3 points has previously been determined as low risk for acute MI (AMI) and optimal for rule-out purposes. The primary outcome was diagnostic performance for ruling out MI, and the secondary outcome was the composite of 90-day AMI or all-cause death.
Results: In OUT-ACS, 3.6% of patients had an AMI (median age 56 years (45-68); 47.7% female), and 3% in TRACE (median age 48 years (32-67); 56.9% female). PreHEAR identified 49.3% (OUT-ACS) and 82.7% (TRACE) as low risk, while preHEART identified 33.6% (OUT-ACS) as low risk. Sensitivity/specificity for AMI were 63.9% (95% CI 50.6 to 75.8)/49.8% (95% CI 47.3 to 52.7) (OUT-ACS) and 65% (95% CI 40.8 to 84.6)/84.2% (95% CI 81.1 to 86.9) (TRACE) for preHEAR and 93.4% (95% CI 84.1 to 98.2)/34.6% (95% CI 32.2 to 37) for preHEART. For the secondary outcome, similar diagnostic performance metrics were found. There were four missed AMI cases in the low-risk preHEART group, who were all female.
Conclusion: Neither the preHEAR nor preHEART scores provide sufficient rule out safety in emergency primary care and may particularly underestimate AMI risk in females.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


