Osama Amin, Ahmed Alaarag, Haidy Khattab, Mahmoud Abou-Omar
{"title":"非瓣膜性心房颤动左房重构参数与脑利钠肽水平。","authors":"Osama Amin, Ahmed Alaarag, Haidy Khattab, Mahmoud Abou-Omar","doi":"10.37616/2212-5043.1446","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Left atrium (LA) remodeling, categorized by functional and structural variations, is predominant in heart failure with preserved ejection fraction (HFpEF) and atrial fibrillation (AF). Brain natriuretic peptide (BNP) levels, implying atrial strain, may lead management by indicating LA remodeling severity. This study was instructed to correlate BNP levels with LA volume index (LAVI) in HFpEF patients with nonvalvular AF against sinus rhythm (SR), to evaluate diagnostic implications.</p><p><strong>Methods: </strong>This two-center, observational, cross-sectional study (April 2023-October 2024) registered 340 patients with de novo HFpEF (140 AF, 200 SR). Patients with left ventricular ejection fraction (LVEF) less than 50 %, valvular disease, or acute conditions were excluded. BNP was measured using enzyme-linked immunosorbent assay and categorized as low (≤200 pg/mL), moderate-high (>200-400 pg/mL), or high (≥400 pg/mL). LAVI was calculated via echocardiography per American Society of Echocardiography (ASE) guidelines, categorized as normal (16-34 mL/m<sup>2</sup>), mildly abnormal (35-41 mL/m<sup>2</sup>), moderately abnormal (42-48 mL/m<sup>2</sup>), or severely abnormal (more than or equal to 49 mL/m<sup>2</sup>). Spearman correlation, multivariate regression, and subgroup analyses by gender, age, and comorbidities were used to assess the associations.</p><p><strong>Results: </strong>AF patients had higher BNP (470 ± 280 vs. 400 ± 211 pg/mL, P = 0.013) and LAVI (60.4 ± 19.0 vs. 54.8 ± 22.0 mL/m<sup>2</sup>, P < 0.001). Paradoxically, AF patients with low BNP (≤200 pg/mL) showed higher LAVI (58 ± 22.0 vs. 54 ± 28.9 mL/m<sup>2</sup>, P < 0.001) and worse New York Heart Association (NYHA) class IV symptoms (48.6 % vs. 35.4 % in SR). A negative correlation between BNP and severely abnormal LAVI (≥49 mL/m<sup>2</sup>) was observed in AF (r = -0.66, P < 0.0001), contrasting with a positive correlation in SR (r = 0.78, P = 0.001). BMI, eGFR, and severely abnormal LAVI were independent predictors (P = 0.004, 0.026, <0.001). Subgroup analyses showed no significant influence of age, gender, or comorbidities.</p><p><strong>Conclusion: </strong>In HFpEF, low BNP levels in AF patients are paradoxically associated with severe LA remodeling and worse symptoms, unlike in SR. BNP interpretation should integrate clinical, echocardiographic, and strain data, particularly in AF, high BMI, or kidney disease, to optimize management.</p>","PeriodicalId":17319,"journal":{"name":"Journal of the Saudi Heart Association","volume":"37 3","pages":"8"},"PeriodicalIF":1.3000,"publicationDate":"2025-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303056/pdf/","citationCount":"0","resultStr":"{\"title\":\"Left Atrial Remodeling Parameters and Brain Natriuretic Peptide Levels in Nonvalvular Atrial Fibrillation.\",\"authors\":\"Osama Amin, Ahmed Alaarag, Haidy Khattab, Mahmoud Abou-Omar\",\"doi\":\"10.37616/2212-5043.1446\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Left atrium (LA) remodeling, categorized by functional and structural variations, is predominant in heart failure with preserved ejection fraction (HFpEF) and atrial fibrillation (AF). Brain natriuretic peptide (BNP) levels, implying atrial strain, may lead management by indicating LA remodeling severity. This study was instructed to correlate BNP levels with LA volume index (LAVI) in HFpEF patients with nonvalvular AF against sinus rhythm (SR), to evaluate diagnostic implications.</p><p><strong>Methods: </strong>This two-center, observational, cross-sectional study (April 2023-October 2024) registered 340 patients with de novo HFpEF (140 AF, 200 SR). Patients with left ventricular ejection fraction (LVEF) less than 50 %, valvular disease, or acute conditions were excluded. BNP was measured using enzyme-linked immunosorbent assay and categorized as low (≤200 pg/mL), moderate-high (>200-400 pg/mL), or high (≥400 pg/mL). LAVI was calculated via echocardiography per American Society of Echocardiography (ASE) guidelines, categorized as normal (16-34 mL/m<sup>2</sup>), mildly abnormal (35-41 mL/m<sup>2</sup>), moderately abnormal (42-48 mL/m<sup>2</sup>), or severely abnormal (more than or equal to 49 mL/m<sup>2</sup>). Spearman correlation, multivariate regression, and subgroup analyses by gender, age, and comorbidities were used to assess the associations.</p><p><strong>Results: </strong>AF patients had higher BNP (470 ± 280 vs. 400 ± 211 pg/mL, P = 0.013) and LAVI (60.4 ± 19.0 vs. 54.8 ± 22.0 mL/m<sup>2</sup>, P < 0.001). Paradoxically, AF patients with low BNP (≤200 pg/mL) showed higher LAVI (58 ± 22.0 vs. 54 ± 28.9 mL/m<sup>2</sup>, P < 0.001) and worse New York Heart Association (NYHA) class IV symptoms (48.6 % vs. 35.4 % in SR). A negative correlation between BNP and severely abnormal LAVI (≥49 mL/m<sup>2</sup>) was observed in AF (r = -0.66, P < 0.0001), contrasting with a positive correlation in SR (r = 0.78, P = 0.001). BMI, eGFR, and severely abnormal LAVI were independent predictors (P = 0.004, 0.026, <0.001). Subgroup analyses showed no significant influence of age, gender, or comorbidities.</p><p><strong>Conclusion: </strong>In HFpEF, low BNP levels in AF patients are paradoxically associated with severe LA remodeling and worse symptoms, unlike in SR. BNP interpretation should integrate clinical, echocardiographic, and strain data, particularly in AF, high BMI, or kidney disease, to optimize management.</p>\",\"PeriodicalId\":17319,\"journal\":{\"name\":\"Journal of the Saudi Heart Association\",\"volume\":\"37 3\",\"pages\":\"8\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-07-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303056/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Saudi Heart Association\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.37616/2212-5043.1446\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Saudi Heart Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37616/2212-5043.1446","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:左心房(LA)重构,根据功能和结构变化分类,主要发生在心力衰竭伴保留射血分数(HFpEF)和心房颤动(AF)。脑钠肽(BNP)水平,暗示心房劳损,可能通过指示LA重塑的严重程度来指导管理。本研究旨在将HFpEF合并非瓣膜性房颤反窦性心律(SR)患者的BNP水平与LA容积指数(LAVI)联系起来,以评估其诊断意义。方法:这项双中心、观察性、横断面研究(2023年4月- 2024年10月)登记了340例新发HFpEF患者(140例AF, 200例SR)。排除左心室射血分数(LVEF)小于50%、瓣膜疾病或急性疾病的患者。采用酶联免疫吸附法测定BNP,并将其分为低(≤200 pg/mL)、中高(200-400 pg/mL)和高(≥400 pg/mL)。LAVI根据美国超声心动图学会(ASE)指南通过超声心动图计算,分为正常(16-34 mL/m2)、轻度异常(35-41 mL/m2)、中度异常(42-48 mL/m2)或严重异常(大于或等于49 mL/m2)。采用Spearman相关、多变量回归和按性别、年龄和合并症划分的亚组分析来评估相关性。结果:AF患者BNP升高(470±280比400±211 pg/mL, P = 0.013), LAVI升高(60.4±19.0比54.8±22.0 mL/m2, P < 0.001)。矛盾的是,低BNP(≤200 pg/mL)的房颤患者LAVI更高(58±22.0 vs. 54±28.9 mL/m2, P < 0.001),纽约心脏协会(NYHA) IV类症状更差(48.6% vs. 35.4% SR)。AF患者BNP与严重异常的LAVI(≥49 mL/m2)呈负相关(r = -0.66, P < 0.0001), SR患者BNP与严重异常的LAVI呈正相关(r = 0.78, P = 0.001)。BMI、eGFR和严重异常的LAVI是独立的预测因子(P = 0.004, 0.026)。结论:在HFpEF中,房颤患者的低BNP水平与严重的LA重塑和更严重的症状矛盾地相关,这与老年房颤不同。BNP的解释应结合临床、超声心动图和应变数据,特别是房颤、高BMI或肾脏疾病,以优化管理。
Left Atrial Remodeling Parameters and Brain Natriuretic Peptide Levels in Nonvalvular Atrial Fibrillation.
Objectives: Left atrium (LA) remodeling, categorized by functional and structural variations, is predominant in heart failure with preserved ejection fraction (HFpEF) and atrial fibrillation (AF). Brain natriuretic peptide (BNP) levels, implying atrial strain, may lead management by indicating LA remodeling severity. This study was instructed to correlate BNP levels with LA volume index (LAVI) in HFpEF patients with nonvalvular AF against sinus rhythm (SR), to evaluate diagnostic implications.
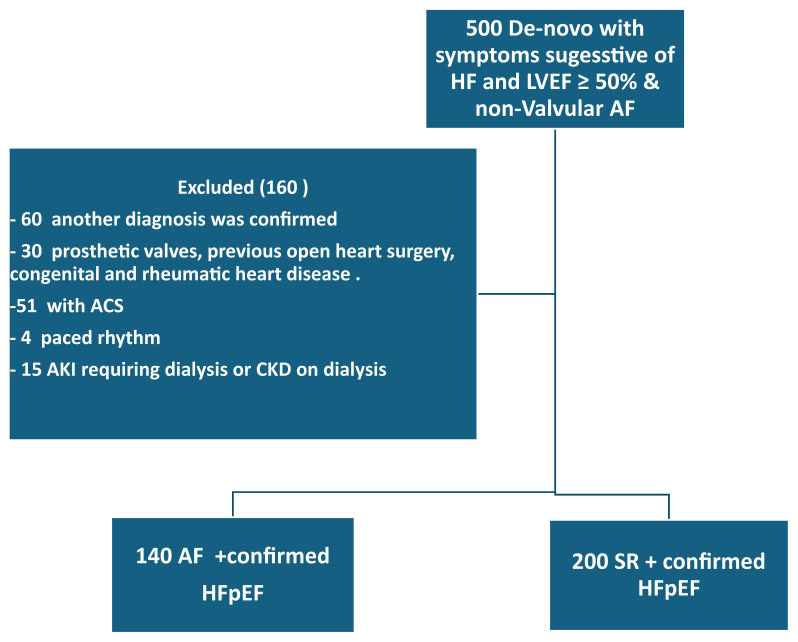
Methods: This two-center, observational, cross-sectional study (April 2023-October 2024) registered 340 patients with de novo HFpEF (140 AF, 200 SR). Patients with left ventricular ejection fraction (LVEF) less than 50 %, valvular disease, or acute conditions were excluded. BNP was measured using enzyme-linked immunosorbent assay and categorized as low (≤200 pg/mL), moderate-high (>200-400 pg/mL), or high (≥400 pg/mL). LAVI was calculated via echocardiography per American Society of Echocardiography (ASE) guidelines, categorized as normal (16-34 mL/m2), mildly abnormal (35-41 mL/m2), moderately abnormal (42-48 mL/m2), or severely abnormal (more than or equal to 49 mL/m2). Spearman correlation, multivariate regression, and subgroup analyses by gender, age, and comorbidities were used to assess the associations.
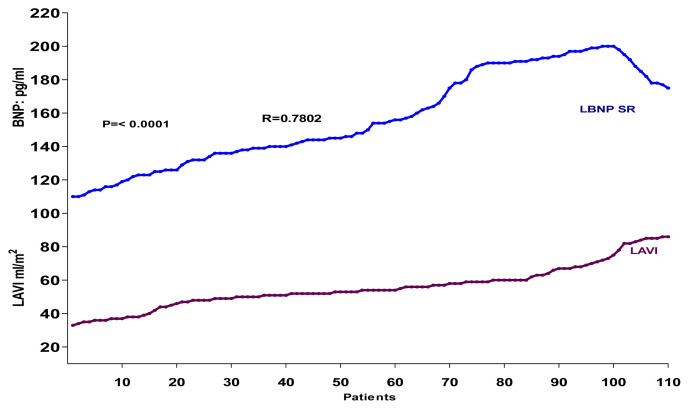
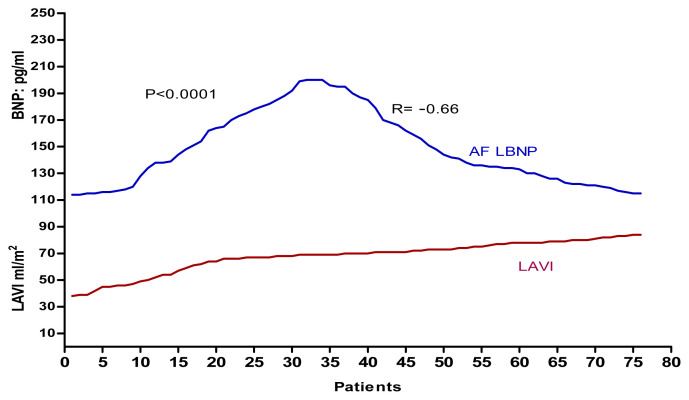
Results: AF patients had higher BNP (470 ± 280 vs. 400 ± 211 pg/mL, P = 0.013) and LAVI (60.4 ± 19.0 vs. 54.8 ± 22.0 mL/m2, P < 0.001). Paradoxically, AF patients with low BNP (≤200 pg/mL) showed higher LAVI (58 ± 22.0 vs. 54 ± 28.9 mL/m2, P < 0.001) and worse New York Heart Association (NYHA) class IV symptoms (48.6 % vs. 35.4 % in SR). A negative correlation between BNP and severely abnormal LAVI (≥49 mL/m2) was observed in AF (r = -0.66, P < 0.0001), contrasting with a positive correlation in SR (r = 0.78, P = 0.001). BMI, eGFR, and severely abnormal LAVI were independent predictors (P = 0.004, 0.026, <0.001). Subgroup analyses showed no significant influence of age, gender, or comorbidities.
Conclusion: In HFpEF, low BNP levels in AF patients are paradoxically associated with severe LA remodeling and worse symptoms, unlike in SR. BNP interpretation should integrate clinical, echocardiographic, and strain data, particularly in AF, high BMI, or kidney disease, to optimize management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


