Luis Gajate Martín, Inés de la Hoz, María Martín, Cristina Fernández, Ascensión Martín Grande, Diego Parise, Judith Villahoz, María Gómez, Mercedes Espiño, Oscar Pastor, Miguel Ángel Rodríguez Gandía, Javier Nuño
{"title":"抗坏血酸预防肝移植后再灌注综合征的随机试验。","authors":"Luis Gajate Martín, Inés de la Hoz, María Martín, Cristina Fernández, Ascensión Martín Grande, Diego Parise, Judith Villahoz, María Gómez, Mercedes Espiño, Oscar Pastor, Miguel Ángel Rodríguez Gandía, Javier Nuño","doi":"10.1097/HC9.0000000000000777","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Post-reperfusion syndrome (PRS) is a critical hemodynamic complication during liver transplantation, characterized by a significant drop in mean arterial pressure and associated with increased morbidity and mortality, systemic inflammation, and ischemia-reperfusion injury. Ascorbic acid (AA), with its antioxidant and anti-inflammatory properties, has been proposed as a potential therapeutic intervention.</p><p><strong>Methods: </strong>A single-center, double-blind, randomized controlled trial was conducted at the Hospital Universitario Ramón y Cajal, Madrid. Patients undergoing liver transplantation were randomly assigned to receive either 1500 mg of intravenous AA during the anhepatic phase (vitamin C-treated group) or 0.9% saline as a placebo (control group). The primary endpoint was PRS incidence. The secondary outcomes included inflammatory cytokine levels, postoperative renal function, and patient/graft survival.</p><p><strong>Results: </strong>Thirty-nine patients were randomized (20 controls and 19 AA-treated patients). The incidence of PRS was 30% in the control group and 10.5% in the AA group (p=0.235). Postoperative renal failure occurred more frequently in the AA group (68.4%) than in the control group (35%) (p=0.037). Four AA-treated patients (21.1%) required re-transplantation. No significant differences in cytokine levels were observed between the groups, although increases in IL-6, IL-8, and IL-10 levels were noted in patients with PRS, suggesting a stronger inflammatory response.</p><p><strong>Conclusions: </strong>AA supplementation demonstrated a noticeable trend toward reducing PRS during liver transplantation, although this was not statistically significant. An increase in renal failure and the need for re-transplantation were observed in the AA-treated group. Although the study suggests potential benefits, its small sample size limits the conclusions, pointing to the need for larger multicenter trials to determine the optimal dosage and timing.</p>","PeriodicalId":12978,"journal":{"name":"Hepatology Communications","volume":"9 8","pages":""},"PeriodicalIF":5.6000,"publicationDate":"2025-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12306706/pdf/","citationCount":"0","resultStr":"{\"title\":\"A randomized trial of ascorbic acid for the prevention of post-reperfusion syndrome during liver transplantation.\",\"authors\":\"Luis Gajate Martín, Inés de la Hoz, María Martín, Cristina Fernández, Ascensión Martín Grande, Diego Parise, Judith Villahoz, María Gómez, Mercedes Espiño, Oscar Pastor, Miguel Ángel Rodríguez Gandía, Javier Nuño\",\"doi\":\"10.1097/HC9.0000000000000777\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Post-reperfusion syndrome (PRS) is a critical hemodynamic complication during liver transplantation, characterized by a significant drop in mean arterial pressure and associated with increased morbidity and mortality, systemic inflammation, and ischemia-reperfusion injury. Ascorbic acid (AA), with its antioxidant and anti-inflammatory properties, has been proposed as a potential therapeutic intervention.</p><p><strong>Methods: </strong>A single-center, double-blind, randomized controlled trial was conducted at the Hospital Universitario Ramón y Cajal, Madrid. Patients undergoing liver transplantation were randomly assigned to receive either 1500 mg of intravenous AA during the anhepatic phase (vitamin C-treated group) or 0.9% saline as a placebo (control group). The primary endpoint was PRS incidence. The secondary outcomes included inflammatory cytokine levels, postoperative renal function, and patient/graft survival.</p><p><strong>Results: </strong>Thirty-nine patients were randomized (20 controls and 19 AA-treated patients). The incidence of PRS was 30% in the control group and 10.5% in the AA group (p=0.235). Postoperative renal failure occurred more frequently in the AA group (68.4%) than in the control group (35%) (p=0.037). Four AA-treated patients (21.1%) required re-transplantation. No significant differences in cytokine levels were observed between the groups, although increases in IL-6, IL-8, and IL-10 levels were noted in patients with PRS, suggesting a stronger inflammatory response.</p><p><strong>Conclusions: </strong>AA supplementation demonstrated a noticeable trend toward reducing PRS during liver transplantation, although this was not statistically significant. An increase in renal failure and the need for re-transplantation were observed in the AA-treated group. Although the study suggests potential benefits, its small sample size limits the conclusions, pointing to the need for larger multicenter trials to determine the optimal dosage and timing.</p>\",\"PeriodicalId\":12978,\"journal\":{\"name\":\"Hepatology Communications\",\"volume\":\"9 8\",\"pages\":\"\"},\"PeriodicalIF\":5.6000,\"publicationDate\":\"2025-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12306706/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hepatology Communications\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/HC9.0000000000000777\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatology Communications","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/HC9.0000000000000777","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:再灌注综合征(PRS)是肝移植过程中重要的血流动力学并发症,其特征是平均动脉压显著下降,与发病率和死亡率增加、全身炎症和缺血再灌注损伤相关。抗坏血酸(AA)具有抗氧化和抗炎的特性,被认为是一种潜在的治疗干预手段。方法:在马德里卡哈尔医院(Ramón y Cajal)进行一项单中心、双盲、随机对照试验。接受肝移植的患者被随机分配在无肝期接受1500mg静脉注射AA(维生素c治疗组)或0.9%生理盐水作为安慰剂(对照组)。主要终点为PRS发生率。次要结局包括炎症细胞因子水平、术后肾功能和患者/移植物存活。结果:39例患者随机分组(对照组20例,aa组19例)。对照组PRS发生率为30%,AA组为10.5% (p=0.235)。AA组术后肾功能衰竭发生率(68.4%)高于对照组(35%)(p=0.037)。4例接受aa治疗的患者(21.1%)需要再次移植。两组间细胞因子水平无显著差异,但PRS患者IL-6、IL-8和IL-10水平升高,提示炎症反应更强。结论:肝移植期间补充AA可显著降低PRS,但无统计学意义。在aa治疗组中观察到肾功能衰竭的增加和再次移植的需要。尽管该研究显示了潜在的益处,但其样本量小限制了结论,指出需要更大规模的多中心试验来确定最佳剂量和时间。
A randomized trial of ascorbic acid for the prevention of post-reperfusion syndrome during liver transplantation.
Background: Post-reperfusion syndrome (PRS) is a critical hemodynamic complication during liver transplantation, characterized by a significant drop in mean arterial pressure and associated with increased morbidity and mortality, systemic inflammation, and ischemia-reperfusion injury. Ascorbic acid (AA), with its antioxidant and anti-inflammatory properties, has been proposed as a potential therapeutic intervention.
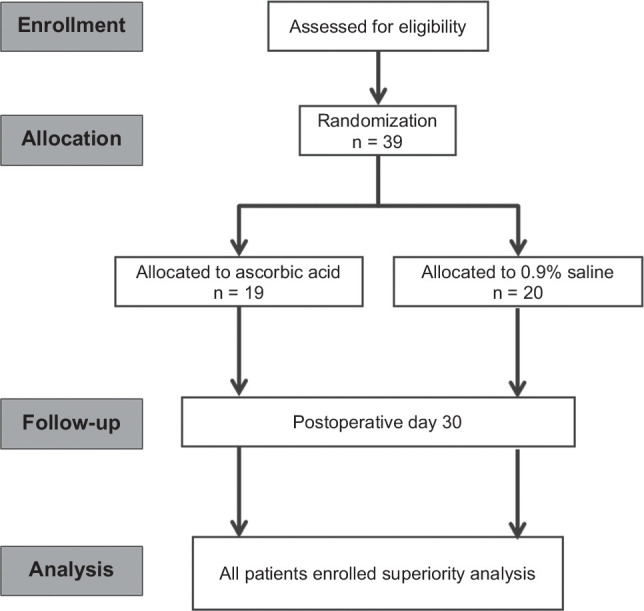
Methods: A single-center, double-blind, randomized controlled trial was conducted at the Hospital Universitario Ramón y Cajal, Madrid. Patients undergoing liver transplantation were randomly assigned to receive either 1500 mg of intravenous AA during the anhepatic phase (vitamin C-treated group) or 0.9% saline as a placebo (control group). The primary endpoint was PRS incidence. The secondary outcomes included inflammatory cytokine levels, postoperative renal function, and patient/graft survival.
Results: Thirty-nine patients were randomized (20 controls and 19 AA-treated patients). The incidence of PRS was 30% in the control group and 10.5% in the AA group (p=0.235). Postoperative renal failure occurred more frequently in the AA group (68.4%) than in the control group (35%) (p=0.037). Four AA-treated patients (21.1%) required re-transplantation. No significant differences in cytokine levels were observed between the groups, although increases in IL-6, IL-8, and IL-10 levels were noted in patients with PRS, suggesting a stronger inflammatory response.
Conclusions: AA supplementation demonstrated a noticeable trend toward reducing PRS during liver transplantation, although this was not statistically significant. An increase in renal failure and the need for re-transplantation were observed in the AA-treated group. Although the study suggests potential benefits, its small sample size limits the conclusions, pointing to the need for larger multicenter trials to determine the optimal dosage and timing.
期刊介绍:
Hepatology Communications is a peer-reviewed, online-only, open access journal for fast dissemination of high quality basic, translational, and clinical research in hepatology. Hepatology Communications maintains high standard and rigorous peer review. Because of its open access nature, authors retain the copyright to their works, all articles are immediately available and free to read and share, and it is fully compliant with funder and institutional mandates. The journal is committed to fast publication and author satisfaction.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


