{"title":"一项回顾性队列研究表明,年龄增加、神经侵犯、外血管侵犯和局部晚期直肠癌的短期放疗与肿瘤消退减少有关。","authors":"O F Johnsen, R Riis, S Meltzer, K M Augestad","doi":"10.1007/s10151-025-03180-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We investigated factors associated with pathologic complete response (pCR) and tumor regression grade (TRG) on the basis of clinical and pathological variables and their impact on cancer-free survival (CFS) after surgery for locally advanced rectal cancer (LARC).</p><p><strong>Methods: </strong>All patients with LARC undergoing neoadjuvant treatment before curative total mesorectal excision surgery were included in a prospective institutional database connected to the National Mortality Registry. One-way analysis of variance and Pearson's chi-squared test were utilized to compare TRG groups. The Kaplan-Meier method and regression models were used to evaluate CFS, radiation modality, and staging factors.</p><p><strong>Results: </strong>Of 700 patients operated on for rectal cancer between 2014 and 2024, 159 (22.7%) had LARC without known systemic cancer. Twenty-seven patients had pCR (TRG 0, 17.0%), 46 TRG 1 (29.0%), 70 TRG 2 (44.0%), and 16 TRG 3 (10%). Poor tumor regression was associated with increasing age (p = 0.009), vascular (p < 0.001) and neural invasion (p = 0.005), less differentiated tumors (p < 0.001), short-course 5 Gy × 5 (p < 0.001) rather than long-course 2 Gy × 25 radiotherapy, and omission of neoadjuvant chemotherapy (p < 0.001). Older age was a predictor of short-course radiotherapy and omission of chemotherapy (p < 0.001). Follow-up time was 46.6 months (IQR 20-80.3 months). No differences were found in CFS between TRG groups 0-3 (p = 0.18), however pCR was associated with improved CFS (p = 0.047).</p><p><strong>Conclusions: </strong>Decreased tumor regression was associated with reduced radiotherapy and chemotherapy, neural and vascular invasion, poor differentiation, and increasing age. The latter may reflect reduced application of neoadjuvant treatment in older patients. Complete responders experienced increased cancer-free survival.</p>","PeriodicalId":51192,"journal":{"name":"Techniques in Coloproctology","volume":"29 1","pages":"152"},"PeriodicalIF":2.9000,"publicationDate":"2025-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12301277/pdf/","citationCount":"0","resultStr":"{\"title\":\"Increasing age, neural invasion, extramural vascular invasion, and short-course radiotherapy in locally advanced rectal cancer are associated with decreased tumor regression: a retrospective cohort study.\",\"authors\":\"O F Johnsen, R Riis, S Meltzer, K M Augestad\",\"doi\":\"10.1007/s10151-025-03180-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>We investigated factors associated with pathologic complete response (pCR) and tumor regression grade (TRG) on the basis of clinical and pathological variables and their impact on cancer-free survival (CFS) after surgery for locally advanced rectal cancer (LARC).</p><p><strong>Methods: </strong>All patients with LARC undergoing neoadjuvant treatment before curative total mesorectal excision surgery were included in a prospective institutional database connected to the National Mortality Registry. One-way analysis of variance and Pearson's chi-squared test were utilized to compare TRG groups. The Kaplan-Meier method and regression models were used to evaluate CFS, radiation modality, and staging factors.</p><p><strong>Results: </strong>Of 700 patients operated on for rectal cancer between 2014 and 2024, 159 (22.7%) had LARC without known systemic cancer. Twenty-seven patients had pCR (TRG 0, 17.0%), 46 TRG 1 (29.0%), 70 TRG 2 (44.0%), and 16 TRG 3 (10%). Poor tumor regression was associated with increasing age (p = 0.009), vascular (p < 0.001) and neural invasion (p = 0.005), less differentiated tumors (p < 0.001), short-course 5 Gy × 5 (p < 0.001) rather than long-course 2 Gy × 25 radiotherapy, and omission of neoadjuvant chemotherapy (p < 0.001). Older age was a predictor of short-course radiotherapy and omission of chemotherapy (p < 0.001). Follow-up time was 46.6 months (IQR 20-80.3 months). No differences were found in CFS between TRG groups 0-3 (p = 0.18), however pCR was associated with improved CFS (p = 0.047).</p><p><strong>Conclusions: </strong>Decreased tumor regression was associated with reduced radiotherapy and chemotherapy, neural and vascular invasion, poor differentiation, and increasing age. The latter may reflect reduced application of neoadjuvant treatment in older patients. Complete responders experienced increased cancer-free survival.</p>\",\"PeriodicalId\":51192,\"journal\":{\"name\":\"Techniques in Coloproctology\",\"volume\":\"29 1\",\"pages\":\"152\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12301277/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Techniques in Coloproctology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10151-025-03180-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Techniques in Coloproctology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10151-025-03180-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Increasing age, neural invasion, extramural vascular invasion, and short-course radiotherapy in locally advanced rectal cancer are associated with decreased tumor regression: a retrospective cohort study.
Background: We investigated factors associated with pathologic complete response (pCR) and tumor regression grade (TRG) on the basis of clinical and pathological variables and their impact on cancer-free survival (CFS) after surgery for locally advanced rectal cancer (LARC).
Methods: All patients with LARC undergoing neoadjuvant treatment before curative total mesorectal excision surgery were included in a prospective institutional database connected to the National Mortality Registry. One-way analysis of variance and Pearson's chi-squared test were utilized to compare TRG groups. The Kaplan-Meier method and regression models were used to evaluate CFS, radiation modality, and staging factors.
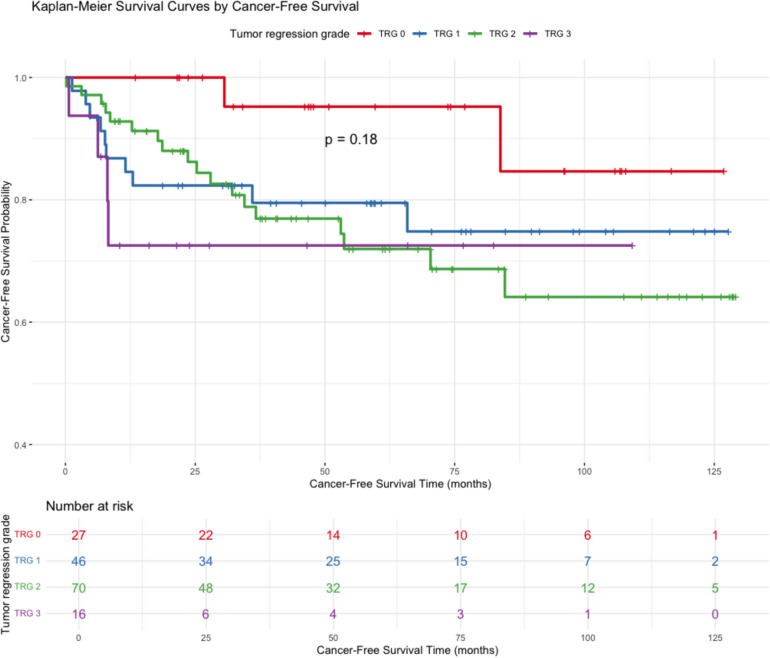
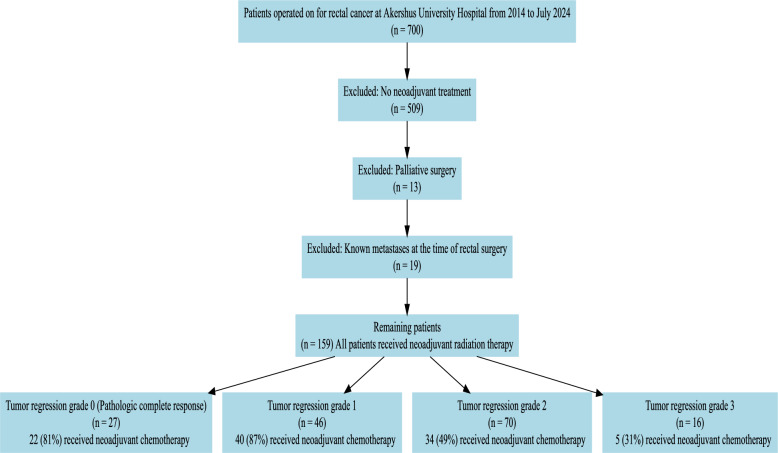
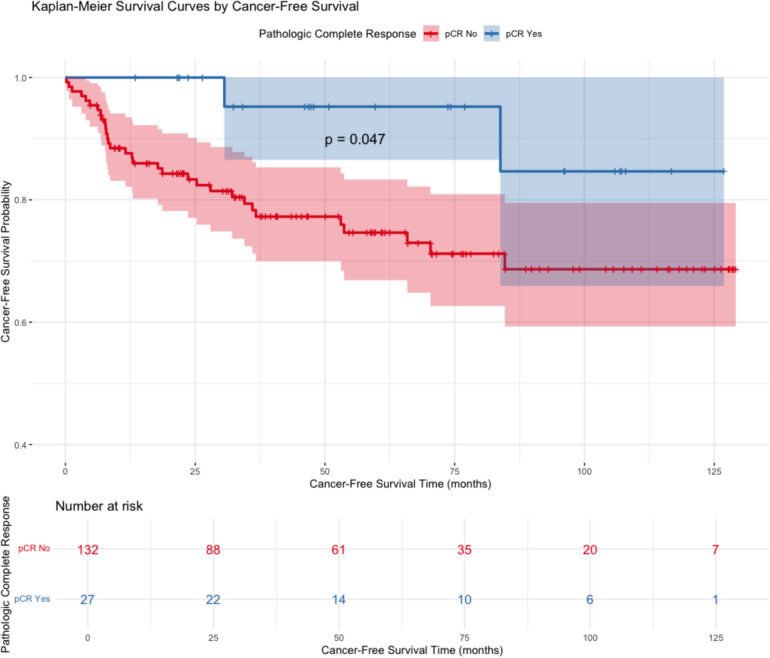
Results: Of 700 patients operated on for rectal cancer between 2014 and 2024, 159 (22.7%) had LARC without known systemic cancer. Twenty-seven patients had pCR (TRG 0, 17.0%), 46 TRG 1 (29.0%), 70 TRG 2 (44.0%), and 16 TRG 3 (10%). Poor tumor regression was associated with increasing age (p = 0.009), vascular (p < 0.001) and neural invasion (p = 0.005), less differentiated tumors (p < 0.001), short-course 5 Gy × 5 (p < 0.001) rather than long-course 2 Gy × 25 radiotherapy, and omission of neoadjuvant chemotherapy (p < 0.001). Older age was a predictor of short-course radiotherapy and omission of chemotherapy (p < 0.001). Follow-up time was 46.6 months (IQR 20-80.3 months). No differences were found in CFS between TRG groups 0-3 (p = 0.18), however pCR was associated with improved CFS (p = 0.047).
Conclusions: Decreased tumor regression was associated with reduced radiotherapy and chemotherapy, neural and vascular invasion, poor differentiation, and increasing age. The latter may reflect reduced application of neoadjuvant treatment in older patients. Complete responders experienced increased cancer-free survival.
期刊介绍:
Techniques in Coloproctology is an international journal fully devoted to diagnostic and operative procedures carried out in the management of colorectal diseases. Imaging, clinical physiology, laparoscopy, open abdominal surgery and proctoperineology are the main topics covered by the journal. Reviews, original articles, technical notes and short communications with many detailed illustrations render this publication indispensable for coloproctologists and related specialists. Both surgeons and gastroenterologists are represented on the distinguished Editorial Board, together with pathologists, radiologists and basic scientists from all over the world. The journal is strongly recommended to those who wish to be updated on recent developments in the field, and improve the standards of their work.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1965 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted. Reports of animal experiments must state that the Principles of Laboratory Animal Care (NIH publication no. 86-23 revised 1985) were followed as were applicable national laws (e.g. the current version of the German Law on the Protection of Animals). The Editor-in-Chief reserves the right to reject manuscripts that do not comply with the above-mentioned requirements. Authors will be held responsible for false statements or for failure to fulfill such requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


