{"title":"在社区居住的老年人中评估SARC-F对可能的肌肉减少症的敏感性:横断面问卷研究。","authors":"David Propst, Lauren Biscardi, Tim Dornemann","doi":"10.2196/54475","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The European Working Group on Sarcopenia in Older People (EWGSOP2) recommends the use of the 5-item SARC-F (strength, assistance with walking, rising from a chair, climbing stairs, and falls) questionnaire by clinicians to screen for probable sarcopenia. The recommended threshold of ≥4 has low sensitivity and high specificity in identifying probable sarcopenia. While this high threshold is effective in excluding clients without probable sarcopenia, challenges exist in using this screening tool to identify clients with low muscle strength.</p><p><strong>Objective: </strong>This study aims to reassess the use of SARC-F in a primary care clinic for the determination of incidence of probable sarcopenia and to evaluate if a handgrip strength test is necessary for its diagnosis.</p><p><strong>Methods: </strong>We screened 204 patients aged ≥65 years (117 men and 87 women) during routine visits with the SARC-F questionnaire. Probable sarcopenia was defined by EWGSOP2 grip strength cut points (≤27 kg for men and ≤16 kg for women). Receiver operating characteristic analysis was performed to identify the SARC-F threshold that best balanced sensitivity and specificity.</p><p><strong>Results: </strong>Probable sarcopenia was present in 12% (n=24) of participants. The mean age (73.9, SD 6.2 years) and mean BMI (29.5, SD 5.8 kg/m²) did not differ significantly by sex; however, men showed a higher mean grip strength (36.3, SD 8.1 kg vs 22.4, SD 5.5 kg; P<.001) and lower mean SARC-F scores (0.9, SD 1.7 vs 1.9, SD 2.3; P<.001). A SARC-F cut point of ≥2 yielded an area under the curve of 0.77 (95% CI 0.67-0.88), with sensitivity of 0.78, specificity of 0.75, accuracy of 0.77, positive predictive value of 0.31, and negative predictive value of 0.96. The grip strength differed significantly between screen-positive and screen-negative groups at both the ≥2 and ≥4 thresholds (P<.001).</p><p><strong>Conclusions: </strong>A SARC- F threshold of ≥2 is recommended as an optimal trade-off between sensitivity and specificity for identifying community-dwelling older adults with probable sarcopenia. This threshold is lower than the currently accepted recommendation of ≥4. Our findings promote the recommendations for early detection and treatment by medical professionals following the EWGSOP2 by improving the ability of clinicians to identify individuals with low muscle strength using this screening procedure.</p>","PeriodicalId":73558,"journal":{"name":"JMIRx med","volume":"6 ","pages":"e54475"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12292031/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessment of SARC-F Sensitivity for Probable Sarcopenia Among Community-Dwelling Older Adults: Cross-Sectional Questionnaire Study.\",\"authors\":\"David Propst, Lauren Biscardi, Tim Dornemann\",\"doi\":\"10.2196/54475\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The European Working Group on Sarcopenia in Older People (EWGSOP2) recommends the use of the 5-item SARC-F (strength, assistance with walking, rising from a chair, climbing stairs, and falls) questionnaire by clinicians to screen for probable sarcopenia. The recommended threshold of ≥4 has low sensitivity and high specificity in identifying probable sarcopenia. While this high threshold is effective in excluding clients without probable sarcopenia, challenges exist in using this screening tool to identify clients with low muscle strength.</p><p><strong>Objective: </strong>This study aims to reassess the use of SARC-F in a primary care clinic for the determination of incidence of probable sarcopenia and to evaluate if a handgrip strength test is necessary for its diagnosis.</p><p><strong>Methods: </strong>We screened 204 patients aged ≥65 years (117 men and 87 women) during routine visits with the SARC-F questionnaire. Probable sarcopenia was defined by EWGSOP2 grip strength cut points (≤27 kg for men and ≤16 kg for women). Receiver operating characteristic analysis was performed to identify the SARC-F threshold that best balanced sensitivity and specificity.</p><p><strong>Results: </strong>Probable sarcopenia was present in 12% (n=24) of participants. The mean age (73.9, SD 6.2 years) and mean BMI (29.5, SD 5.8 kg/m²) did not differ significantly by sex; however, men showed a higher mean grip strength (36.3, SD 8.1 kg vs 22.4, SD 5.5 kg; P<.001) and lower mean SARC-F scores (0.9, SD 1.7 vs 1.9, SD 2.3; P<.001). A SARC-F cut point of ≥2 yielded an area under the curve of 0.77 (95% CI 0.67-0.88), with sensitivity of 0.78, specificity of 0.75, accuracy of 0.77, positive predictive value of 0.31, and negative predictive value of 0.96. The grip strength differed significantly between screen-positive and screen-negative groups at both the ≥2 and ≥4 thresholds (P<.001).</p><p><strong>Conclusions: </strong>A SARC- F threshold of ≥2 is recommended as an optimal trade-off between sensitivity and specificity for identifying community-dwelling older adults with probable sarcopenia. This threshold is lower than the currently accepted recommendation of ≥4. Our findings promote the recommendations for early detection and treatment by medical professionals following the EWGSOP2 by improving the ability of clinicians to identify individuals with low muscle strength using this screening procedure.</p>\",\"PeriodicalId\":73558,\"journal\":{\"name\":\"JMIRx med\",\"volume\":\"6 \",\"pages\":\"e54475\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12292031/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIRx med\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/54475\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIRx med","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/54475","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:欧洲老年人肌肉减少症工作组(EWGSOP2)建议临床医生使用5项SARC-F(力量、行走辅助、从椅子上站起来、爬楼梯和跌倒)问卷来筛查可能的肌肉减少症。推荐阈值≥4在鉴别可能的肌少症时敏感性低,特异性高。虽然这个高阈值在排除可能没有肌肉减少症的患者方面是有效的,但在使用这个筛选工具来识别肌肉力量低的患者方面存在挑战。目的:本研究旨在重新评估SARC-F在初级保健诊所用于确定可能的肌肉减少症发生率的使用,并评估是否有必要进行握力测试以诊断其。方法:我们在常规访问中筛选204例 年龄≥65 岁的患者(117名男性,87名女性),使用SARC-F问卷。根据EWGSOP2握力切点(男性≤27 kg,女性≤16 kg)定义可能的肌肉减少症。进行受试者工作特征分析以确定最佳平衡敏感性和特异性的SARC-F阈值。结果:12% (n=24)的参与者可能存在肌肉减少症。平均年龄(73.9岁,SD 6.2岁)和平均BMI(29.5岁,SD 5.8 kg/m²)在性别上无显著差异;然而,男性的平均握力更高(36.3, SD 8.1 kg vs 22.4,SD 5.5 kg;结论:SARC- F阈值≥2被推荐为识别社区居住老年人可能的肌肉减少症的敏感性和特异性之间的最佳权衡。该阈值低于目前公认的≥4的推荐值。我们的研究结果通过提高临床医生使用EWGSOP2筛查程序识别低肌力个体的能力,促进了医疗专业人员根据EWGSOP2进行早期检测和治疗的建议。
Assessment of SARC-F Sensitivity for Probable Sarcopenia Among Community-Dwelling Older Adults: Cross-Sectional Questionnaire Study.
Background: The European Working Group on Sarcopenia in Older People (EWGSOP2) recommends the use of the 5-item SARC-F (strength, assistance with walking, rising from a chair, climbing stairs, and falls) questionnaire by clinicians to screen for probable sarcopenia. The recommended threshold of ≥4 has low sensitivity and high specificity in identifying probable sarcopenia. While this high threshold is effective in excluding clients without probable sarcopenia, challenges exist in using this screening tool to identify clients with low muscle strength.
Objective: This study aims to reassess the use of SARC-F in a primary care clinic for the determination of incidence of probable sarcopenia and to evaluate if a handgrip strength test is necessary for its diagnosis.
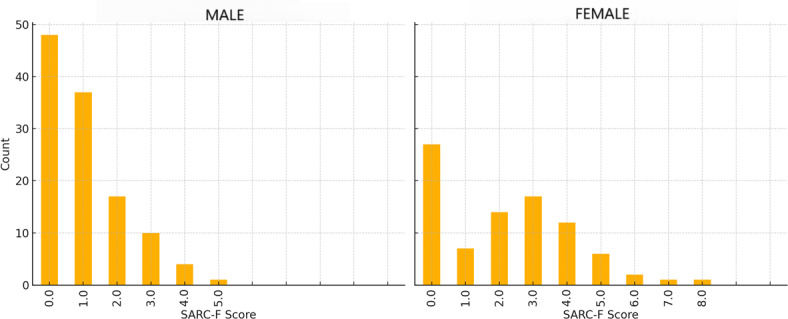
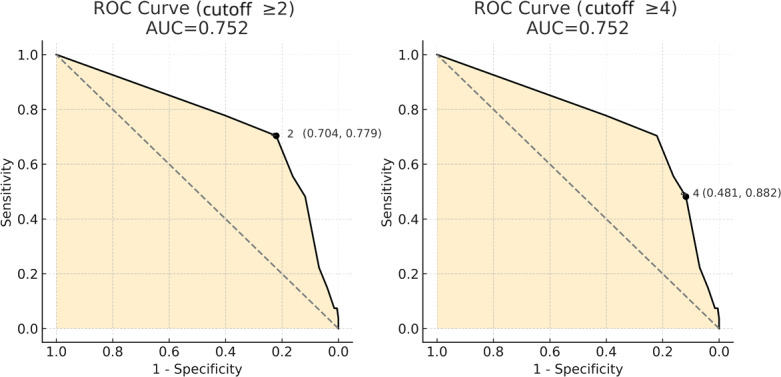
Methods: We screened 204 patients aged ≥65 years (117 men and 87 women) during routine visits with the SARC-F questionnaire. Probable sarcopenia was defined by EWGSOP2 grip strength cut points (≤27 kg for men and ≤16 kg for women). Receiver operating characteristic analysis was performed to identify the SARC-F threshold that best balanced sensitivity and specificity.
Results: Probable sarcopenia was present in 12% (n=24) of participants. The mean age (73.9, SD 6.2 years) and mean BMI (29.5, SD 5.8 kg/m²) did not differ significantly by sex; however, men showed a higher mean grip strength (36.3, SD 8.1 kg vs 22.4, SD 5.5 kg; P<.001) and lower mean SARC-F scores (0.9, SD 1.7 vs 1.9, SD 2.3; P<.001). A SARC-F cut point of ≥2 yielded an area under the curve of 0.77 (95% CI 0.67-0.88), with sensitivity of 0.78, specificity of 0.75, accuracy of 0.77, positive predictive value of 0.31, and negative predictive value of 0.96. The grip strength differed significantly between screen-positive and screen-negative groups at both the ≥2 and ≥4 thresholds (P<.001).
Conclusions: A SARC- F threshold of ≥2 is recommended as an optimal trade-off between sensitivity and specificity for identifying community-dwelling older adults with probable sarcopenia. This threshold is lower than the currently accepted recommendation of ≥4. Our findings promote the recommendations for early detection and treatment by medical professionals following the EWGSOP2 by improving the ability of clinicians to identify individuals with low muscle strength using this screening procedure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


