Melina Bigler, Florian Zacher, Sarah Dräger, Werner C Albrich, Daniel Mäusezahl
{"title":"微生物检测对瑞士军团病抗生素处方的测试和治疗影响:多中心SwissLEGIO研究结果","authors":"Melina Bigler, Florian Zacher, Sarah Dräger, Werner C Albrich, Daniel Mäusezahl","doi":"10.1186/s41479-025-00171-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Legionnaires' disease (LD) is a severe form of primarily community-acquired pneumonia (CAP). To confirm a Legionella infection, microbiological testing is required. The Swiss and European guidelines recommend LD testing for all hospitalised CAP patients. However, the low positivity rate of such routine testing (1.5-3%) raises concerns about its cost-effectiveness and clinical utility. In a setting where routine testing is recommended, this multicentre study evaluated the impact of LD testing on the clinical management of the infection and antimicrobial prescribing.</p><p><strong>Methods: </strong>Data from medical records of 195 community-acquired LD (CALD) patients from 20 Swiss hospitals (August 2022-March 2024) were analysed. We assessed the clinical management of CALD, focusing on the impact of microbiological testing on antibiotic prescribing. The appropriateness of antibiotic choice and duration of treatment was assessed using a standardised pathway analysis approach. Factors associated with unsupported antibiotic prescribing were assessed using mixed-effects logistic regression analysis.</p><p><strong>Results: </strong>Microbiological testing was initiated promptly, with results available within 24 h after presenting to the hospital for 85.1% and within 48 h for 92.3% of patients. Antibiotics with Legionella coverage were initiated in 88.2% of patients within 24 h of admission. A positive Legionella test influenced antibiotic prescribing: 97.9% of patients received antibiotics active against Legionella spp., and 79.6% were prescribed appropriate and targeted monotherapy within 24 h of receiving the test result. Overall, 35.4% of patients were treated with antibiotics for a median of 4 days (IQR 3-4 days) longer than guidelines recommend (defined as > 10 days for immunocompetent or > 21 days for immunocompromised patients). Prolonged treatment was associated with CALD severity and antibiotic use > 2 days postdischarge (proxy for clinical stability reached). 38.5% of patients with impaired renal function received a suboptimal loading dose of levofloxacin.</p><p><strong>Conclusion: </strong>Routine aetiological testing for LD has improved the clinical management of CALD by facilitating rapid detection of CALD cases and timely initiation of appropriate and targeted antibiotic therapy. Future antimicrobial stewardship efforts should sensitise physicians that a shorter duration of antibiotic treatment for CALD of 5 to 7 days according to the latest Swiss CAP guidelines is sufficient and safe.</p>","PeriodicalId":45120,"journal":{"name":"Pneumonia","volume":"17 1","pages":"17"},"PeriodicalIF":6.2000,"publicationDate":"2025-07-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12291349/pdf/","citationCount":"0","resultStr":"{\"title\":\"Test and treat-impact of microbiological testing on antibiotic prescribing for Legionnaires' disease in Switzerland: results of the multicentre SwissLEGIO study.\",\"authors\":\"Melina Bigler, Florian Zacher, Sarah Dräger, Werner C Albrich, Daniel Mäusezahl\",\"doi\":\"10.1186/s41479-025-00171-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Legionnaires' disease (LD) is a severe form of primarily community-acquired pneumonia (CAP). To confirm a Legionella infection, microbiological testing is required. The Swiss and European guidelines recommend LD testing for all hospitalised CAP patients. However, the low positivity rate of such routine testing (1.5-3%) raises concerns about its cost-effectiveness and clinical utility. In a setting where routine testing is recommended, this multicentre study evaluated the impact of LD testing on the clinical management of the infection and antimicrobial prescribing.</p><p><strong>Methods: </strong>Data from medical records of 195 community-acquired LD (CALD) patients from 20 Swiss hospitals (August 2022-March 2024) were analysed. We assessed the clinical management of CALD, focusing on the impact of microbiological testing on antibiotic prescribing. The appropriateness of antibiotic choice and duration of treatment was assessed using a standardised pathway analysis approach. Factors associated with unsupported antibiotic prescribing were assessed using mixed-effects logistic regression analysis.</p><p><strong>Results: </strong>Microbiological testing was initiated promptly, with results available within 24 h after presenting to the hospital for 85.1% and within 48 h for 92.3% of patients. Antibiotics with Legionella coverage were initiated in 88.2% of patients within 24 h of admission. A positive Legionella test influenced antibiotic prescribing: 97.9% of patients received antibiotics active against Legionella spp., and 79.6% were prescribed appropriate and targeted monotherapy within 24 h of receiving the test result. Overall, 35.4% of patients were treated with antibiotics for a median of 4 days (IQR 3-4 days) longer than guidelines recommend (defined as > 10 days for immunocompetent or > 21 days for immunocompromised patients). Prolonged treatment was associated with CALD severity and antibiotic use > 2 days postdischarge (proxy for clinical stability reached). 38.5% of patients with impaired renal function received a suboptimal loading dose of levofloxacin.</p><p><strong>Conclusion: </strong>Routine aetiological testing for LD has improved the clinical management of CALD by facilitating rapid detection of CALD cases and timely initiation of appropriate and targeted antibiotic therapy. Future antimicrobial stewardship efforts should sensitise physicians that a shorter duration of antibiotic treatment for CALD of 5 to 7 days according to the latest Swiss CAP guidelines is sufficient and safe.</p>\",\"PeriodicalId\":45120,\"journal\":{\"name\":\"Pneumonia\",\"volume\":\"17 1\",\"pages\":\"17\"},\"PeriodicalIF\":6.2000,\"publicationDate\":\"2025-07-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12291349/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pneumonia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41479-025-00171-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pneumonia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41479-025-00171-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Test and treat-impact of microbiological testing on antibiotic prescribing for Legionnaires' disease in Switzerland: results of the multicentre SwissLEGIO study.
Background: Legionnaires' disease (LD) is a severe form of primarily community-acquired pneumonia (CAP). To confirm a Legionella infection, microbiological testing is required. The Swiss and European guidelines recommend LD testing for all hospitalised CAP patients. However, the low positivity rate of such routine testing (1.5-3%) raises concerns about its cost-effectiveness and clinical utility. In a setting where routine testing is recommended, this multicentre study evaluated the impact of LD testing on the clinical management of the infection and antimicrobial prescribing.
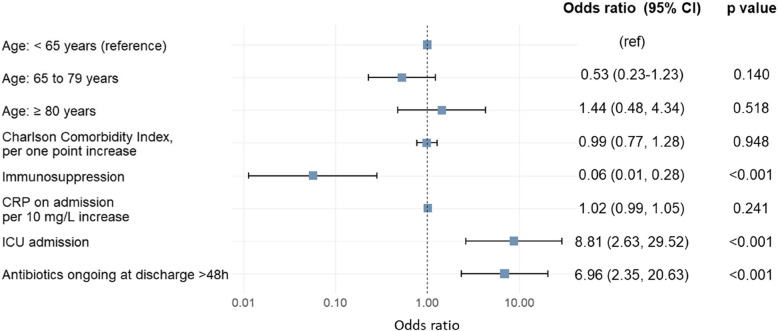
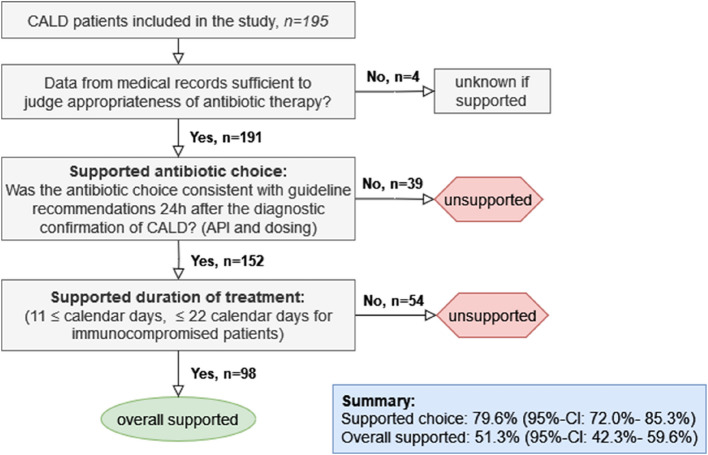
Methods: Data from medical records of 195 community-acquired LD (CALD) patients from 20 Swiss hospitals (August 2022-March 2024) were analysed. We assessed the clinical management of CALD, focusing on the impact of microbiological testing on antibiotic prescribing. The appropriateness of antibiotic choice and duration of treatment was assessed using a standardised pathway analysis approach. Factors associated with unsupported antibiotic prescribing were assessed using mixed-effects logistic regression analysis.
Results: Microbiological testing was initiated promptly, with results available within 24 h after presenting to the hospital for 85.1% and within 48 h for 92.3% of patients. Antibiotics with Legionella coverage were initiated in 88.2% of patients within 24 h of admission. A positive Legionella test influenced antibiotic prescribing: 97.9% of patients received antibiotics active against Legionella spp., and 79.6% were prescribed appropriate and targeted monotherapy within 24 h of receiving the test result. Overall, 35.4% of patients were treated with antibiotics for a median of 4 days (IQR 3-4 days) longer than guidelines recommend (defined as > 10 days for immunocompetent or > 21 days for immunocompromised patients). Prolonged treatment was associated with CALD severity and antibiotic use > 2 days postdischarge (proxy for clinical stability reached). 38.5% of patients with impaired renal function received a suboptimal loading dose of levofloxacin.
Conclusion: Routine aetiological testing for LD has improved the clinical management of CALD by facilitating rapid detection of CALD cases and timely initiation of appropriate and targeted antibiotic therapy. Future antimicrobial stewardship efforts should sensitise physicians that a shorter duration of antibiotic treatment for CALD of 5 to 7 days according to the latest Swiss CAP guidelines is sufficient and safe.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


