{"title":"选择性5 -羟色胺再摄取抑制剂相关颅内出血:药物特异性风险模式和患者水平调节剂。","authors":"Josef Yayan, Kurt Rasche","doi":"10.3390/neurolint17070111","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Selective serotonin reuptake inhibitors (SSRIs) are among the most commonly prescribed antidepressants and are generally considered safe. However, emerging data suggest a potential association with intracranial hemorrhage (ICH), especially among elderly patients and those on anticoagulation.</p><p><strong>Methods: </strong>We conducted a retrospective pharmacovigilance analysis using data from the U.S. Food and Drug Administration's Adverse Event Reporting System (FAERS). Reports up to May 2025 listing an SSRI (sertraline, fluoxetine, paroxetine, escitalopram, citalopram, or fluvoxamine) as a suspect or interacting drug and involving an ICH event were included. Disproportionality was assessed using reporting odds ratios (RORs) with 95% confidence intervals.</p><p><strong>Results: </strong>Among 226 eligible ICH cases, sertraline (30.5%), paroxetine (28.8%), and fluoxetine (27.9%) were most frequently implicated. Sertraline showed a strong signal for cerebral hemorrhage (ROR = 4.97), while fluoxetine was associated with subarachnoid hemorrhage (ROR = 4.51). Sertraline had a pronounced signal among patients aged >60 years (ROR = 7.92) and in combination with anticoagulants (ROR = 9.56). Fluoxetine was underrepresented in elderly cases. Given the very small number of fluvoxamine-related cases (n = 2), interpretation should be cautious due to limited statistical power. Gender-stratified analyses showed female predominance in sertraline-related ICH and male predominance for paroxetine. Citalopram demonstrated a potentially protective profile with inverse association with cerebral hemorrhage.</p><p><strong>Conclusions: </strong>This study highlights significant differences in ICH reporting patterns across SSRIs, modified by patient age, gender, and co-medication. These findings underscore the need for individualized SSRI prescribing, particularly in patients receiving anticoagulant therapy particularly in elderly patients and those receiving anticoagulant therapy, where sertraline and fluoxetine may pose increased risk.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"17 7","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12299848/pdf/","citationCount":"0","resultStr":"{\"title\":\"Selective Serotonin Reuptake Inhibitor-Associated Intracranial Hemorrhage: Drug-Specific Risk Patterns and Patient-Level Modifiers.\",\"authors\":\"Josef Yayan, Kurt Rasche\",\"doi\":\"10.3390/neurolint17070111\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Selective serotonin reuptake inhibitors (SSRIs) are among the most commonly prescribed antidepressants and are generally considered safe. However, emerging data suggest a potential association with intracranial hemorrhage (ICH), especially among elderly patients and those on anticoagulation.</p><p><strong>Methods: </strong>We conducted a retrospective pharmacovigilance analysis using data from the U.S. Food and Drug Administration's Adverse Event Reporting System (FAERS). Reports up to May 2025 listing an SSRI (sertraline, fluoxetine, paroxetine, escitalopram, citalopram, or fluvoxamine) as a suspect or interacting drug and involving an ICH event were included. Disproportionality was assessed using reporting odds ratios (RORs) with 95% confidence intervals.</p><p><strong>Results: </strong>Among 226 eligible ICH cases, sertraline (30.5%), paroxetine (28.8%), and fluoxetine (27.9%) were most frequently implicated. Sertraline showed a strong signal for cerebral hemorrhage (ROR = 4.97), while fluoxetine was associated with subarachnoid hemorrhage (ROR = 4.51). Sertraline had a pronounced signal among patients aged >60 years (ROR = 7.92) and in combination with anticoagulants (ROR = 9.56). Fluoxetine was underrepresented in elderly cases. Given the very small number of fluvoxamine-related cases (n = 2), interpretation should be cautious due to limited statistical power. Gender-stratified analyses showed female predominance in sertraline-related ICH and male predominance for paroxetine. Citalopram demonstrated a potentially protective profile with inverse association with cerebral hemorrhage.</p><p><strong>Conclusions: </strong>This study highlights significant differences in ICH reporting patterns across SSRIs, modified by patient age, gender, and co-medication. These findings underscore the need for individualized SSRI prescribing, particularly in patients receiving anticoagulant therapy particularly in elderly patients and those receiving anticoagulant therapy, where sertraline and fluoxetine may pose increased risk.</p>\",\"PeriodicalId\":19130,\"journal\":{\"name\":\"Neurology International\",\"volume\":\"17 7\",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12299848/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/neurolint17070111\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint17070111","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Background: Selective serotonin reuptake inhibitors (SSRIs) are among the most commonly prescribed antidepressants and are generally considered safe. However, emerging data suggest a potential association with intracranial hemorrhage (ICH), especially among elderly patients and those on anticoagulation.
Methods: We conducted a retrospective pharmacovigilance analysis using data from the U.S. Food and Drug Administration's Adverse Event Reporting System (FAERS). Reports up to May 2025 listing an SSRI (sertraline, fluoxetine, paroxetine, escitalopram, citalopram, or fluvoxamine) as a suspect or interacting drug and involving an ICH event were included. Disproportionality was assessed using reporting odds ratios (RORs) with 95% confidence intervals.
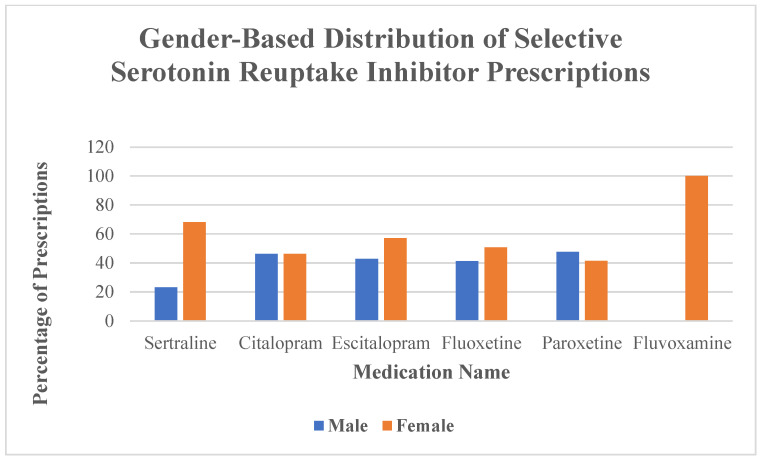
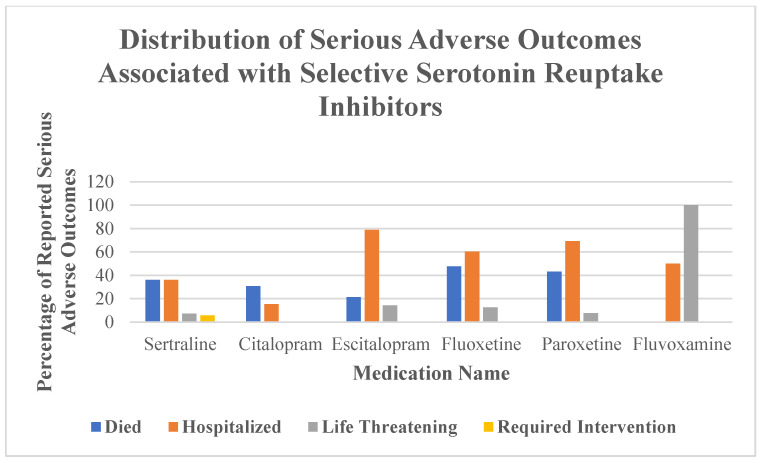
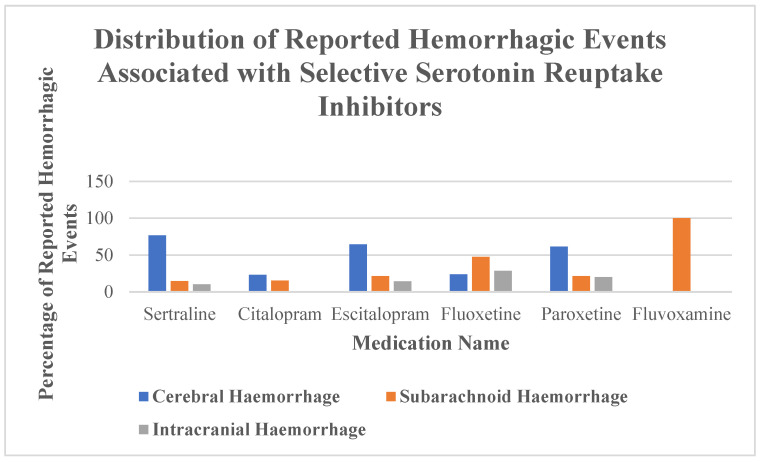
Results: Among 226 eligible ICH cases, sertraline (30.5%), paroxetine (28.8%), and fluoxetine (27.9%) were most frequently implicated. Sertraline showed a strong signal for cerebral hemorrhage (ROR = 4.97), while fluoxetine was associated with subarachnoid hemorrhage (ROR = 4.51). Sertraline had a pronounced signal among patients aged >60 years (ROR = 7.92) and in combination with anticoagulants (ROR = 9.56). Fluoxetine was underrepresented in elderly cases. Given the very small number of fluvoxamine-related cases (n = 2), interpretation should be cautious due to limited statistical power. Gender-stratified analyses showed female predominance in sertraline-related ICH and male predominance for paroxetine. Citalopram demonstrated a potentially protective profile with inverse association with cerebral hemorrhage.
Conclusions: This study highlights significant differences in ICH reporting patterns across SSRIs, modified by patient age, gender, and co-medication. These findings underscore the need for individualized SSRI prescribing, particularly in patients receiving anticoagulant therapy particularly in elderly patients and those receiving anticoagulant therapy, where sertraline and fluoxetine may pose increased risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


