Lisa B E Shields, Vasudeva G Iyer, Yi Ping Zhang, Christopher B Shields
{"title":"10例“伪Wartenberg征”的回顾性分析。","authors":"Lisa B E Shields, Vasudeva G Iyer, Yi Ping Zhang, Christopher B Shields","doi":"10.3390/neurolint17070097","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>The Wartenberg sign is a diagnostic feature of ulnar nerve neuropathy. It results from unbalanced activity of the abductor digiti minimi (ADM) and extensor digiti minimi (EDM) muscles secondary to weakness of the third palmar interosseous muscle. Rarely, this sign may occur in the absence of an underlying ulnar neuropathy, which we refer to as the \"pseudo Wartenberg sign\" (PWS).</p><p><strong>Methods: </strong>This is a retrospective review of 10 patients manifesting an inability to adduct the little finger towards the ring finger with no evidence of an ulnar neuropathy. We describe the clinical and electrodiagnostic (EDX) findings in these patients and discuss the pathophysiologic basis of PWS.</p><p><strong>Results: </strong>The most common cause was an injury in five (50.0%) patients: avulsion of the third volar interosseous muscle in two (20.0%), contracture of the ADM muscle in one (10.0%), and trauma-related dystonia in two (20.0%). The most frequent mechanism of PWS was focal dystonia of specific hand muscles in seven (70.0%) patients. Needle electromyography (EMG) demonstrated no denervation changes in ulnar nerve-innervated hand muscles; the motor and sensory conduction was normal in the ulnar nerve in all patients. Four (40.0%) patients underwent ultrasound studies, with a hyperechoic, avulsed third volar interosseous muscle in one, a hyperechoic and atrophic ADM muscle in one, normal hypothenar and extensor muscles in one, and a normal hypothenar muscle in one.</p><p><strong>Conclusions: </strong>Neurologists, neurosurgeons, and hand and orthopedic surgeons should be aware of the rare cases in which the inability to adduct the little finger may occur in the absence of ulnar neuropathy and look for other causes like avulsion of the third palmar interosseus muscle or focal hand dystonia.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"17 7","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12299210/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Retrospective Study of 10 Patients Exhibiting the \\\"Pseudo Wartenberg Sign\\\".\",\"authors\":\"Lisa B E Shields, Vasudeva G Iyer, Yi Ping Zhang, Christopher B Shields\",\"doi\":\"10.3390/neurolint17070097\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/objectives: </strong>The Wartenberg sign is a diagnostic feature of ulnar nerve neuropathy. It results from unbalanced activity of the abductor digiti minimi (ADM) and extensor digiti minimi (EDM) muscles secondary to weakness of the third palmar interosseous muscle. Rarely, this sign may occur in the absence of an underlying ulnar neuropathy, which we refer to as the \\\"pseudo Wartenberg sign\\\" (PWS).</p><p><strong>Methods: </strong>This is a retrospective review of 10 patients manifesting an inability to adduct the little finger towards the ring finger with no evidence of an ulnar neuropathy. We describe the clinical and electrodiagnostic (EDX) findings in these patients and discuss the pathophysiologic basis of PWS.</p><p><strong>Results: </strong>The most common cause was an injury in five (50.0%) patients: avulsion of the third volar interosseous muscle in two (20.0%), contracture of the ADM muscle in one (10.0%), and trauma-related dystonia in two (20.0%). The most frequent mechanism of PWS was focal dystonia of specific hand muscles in seven (70.0%) patients. Needle electromyography (EMG) demonstrated no denervation changes in ulnar nerve-innervated hand muscles; the motor and sensory conduction was normal in the ulnar nerve in all patients. Four (40.0%) patients underwent ultrasound studies, with a hyperechoic, avulsed third volar interosseous muscle in one, a hyperechoic and atrophic ADM muscle in one, normal hypothenar and extensor muscles in one, and a normal hypothenar muscle in one.</p><p><strong>Conclusions: </strong>Neurologists, neurosurgeons, and hand and orthopedic surgeons should be aware of the rare cases in which the inability to adduct the little finger may occur in the absence of ulnar neuropathy and look for other causes like avulsion of the third palmar interosseus muscle or focal hand dystonia.</p>\",\"PeriodicalId\":19130,\"journal\":{\"name\":\"Neurology International\",\"volume\":\"17 7\",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12299210/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/neurolint17070097\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint17070097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
A Retrospective Study of 10 Patients Exhibiting the "Pseudo Wartenberg Sign".
Background/objectives: The Wartenberg sign is a diagnostic feature of ulnar nerve neuropathy. It results from unbalanced activity of the abductor digiti minimi (ADM) and extensor digiti minimi (EDM) muscles secondary to weakness of the third palmar interosseous muscle. Rarely, this sign may occur in the absence of an underlying ulnar neuropathy, which we refer to as the "pseudo Wartenberg sign" (PWS).
Methods: This is a retrospective review of 10 patients manifesting an inability to adduct the little finger towards the ring finger with no evidence of an ulnar neuropathy. We describe the clinical and electrodiagnostic (EDX) findings in these patients and discuss the pathophysiologic basis of PWS.
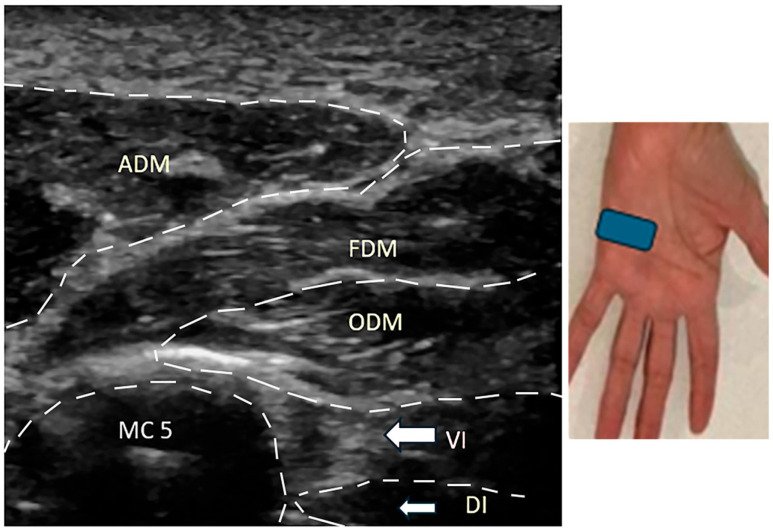
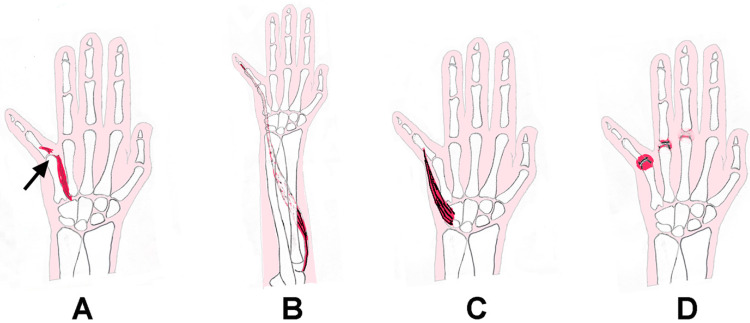
Results: The most common cause was an injury in five (50.0%) patients: avulsion of the third volar interosseous muscle in two (20.0%), contracture of the ADM muscle in one (10.0%), and trauma-related dystonia in two (20.0%). The most frequent mechanism of PWS was focal dystonia of specific hand muscles in seven (70.0%) patients. Needle electromyography (EMG) demonstrated no denervation changes in ulnar nerve-innervated hand muscles; the motor and sensory conduction was normal in the ulnar nerve in all patients. Four (40.0%) patients underwent ultrasound studies, with a hyperechoic, avulsed third volar interosseous muscle in one, a hyperechoic and atrophic ADM muscle in one, normal hypothenar and extensor muscles in one, and a normal hypothenar muscle in one.
Conclusions: Neurologists, neurosurgeons, and hand and orthopedic surgeons should be aware of the rare cases in which the inability to adduct the little finger may occur in the absence of ulnar neuropathy and look for other causes like avulsion of the third palmar interosseus muscle or focal hand dystonia.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


