Naonori Tashiro, Hiroki Nishiwaki, Takashi Ikeda, William M M Levack, Hisashi Noma, Noyuri Yamaji, Erika Ota, Takeshi Hasegawa
{"title":"横膈膜超声在成人机械呼吸机解放中的临床应用:一项系统回顾和荟萃分析。","authors":"Naonori Tashiro, Hiroki Nishiwaki, Takashi Ikeda, William M M Levack, Hisashi Noma, Noyuri Yamaji, Erika Ota, Takeshi Hasegawa","doi":"10.1186/s40560-025-00811-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prolonged mechanical ventilation is associated with an increased incidence of complications and higher mortality rates. Therefore, it is crucial to wean patients from mechanical ventilation as soon as possible. Recently, diaphragmatic ultrasound has been used in this decision-making process. This systematic review evaluated the effectiveness of diaphragmatic ultrasound to improve ventilator liberation outcomes.</p><p><strong>Methods: </strong>We searched three databases - MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. We included randomized control trials that compared the use of diaphragmatic ultrasound to standard care in adult patients on mechanical ventilation via tracheal intubation. We assessed risk of bias for included trials with the Cochrane Risk of Bias Tool and certainty of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation tool. For dichotomous outcomes, we reported risk ratios (RRs) with 95% confidence intervals (CIs). For continuous outcomes, we reported mean differences (MD) with 95% CIs if all retrieved records provide data on the same scale. The primary outcome was incidence of reintubation within 48 h of extubation and the secondary outcomes included duration of mechanical ventilation, incidence of reintubation rate after 48 h, ICU length of stay, and adverse events.</p><p><strong>Results: </strong>We found five relevant randomized controlled trials involving a total of 508 participants on mechanical ventilation in ICU following respiratory failure or surgery. Three studies (268 participants) provided data on the incidence of reintubation within 48 h of extubation. Using diaphragmatic ultrasound to guide extubation decisions led to a significant reduction in the risk of reintubation within 48 h (RR 0.62, 95% CI 0.41 to 0.95, low certainty of evidence). No significant differences were found in the duration of mechanical ventilation (MD - 1.39 h, 95% CI - 17.5 to 14.71 h, three studies, 268 participants, very low certainty of evidence) or reintubation after 48 h (RR 0.38, 95% CI 0.11-1.29, two studies, 240 participants, moderate certainty of evidence). However, ICU length of stay was significantly reduced in the diaphragmatic ultrasound group (MD - 1.0 days, 95% CI - 1.74 to - 0.26 days, one study, 130 participants, low certainty of evidence).</p><p><strong>Conclusion: </strong>Using diaphragmatic ultrasound in addition to standard clinical criteria to guide decisions around ventilator use and liberation resulted in a reduced risk of reintubation within 48 h of extubation when compared to standard clinical criteria alone.</p><p><strong>Systematic review registration: </strong>This systematic review was registered with the Open Science Framework: https://osf.io/cn8xf .</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"13 1","pages":"40"},"PeriodicalIF":4.7000,"publicationDate":"2025-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288223/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical utility of diaphragmatic ultrasound for mechanical ventilator liberation in adults: a systematic review and meta-analysis.\",\"authors\":\"Naonori Tashiro, Hiroki Nishiwaki, Takashi Ikeda, William M M Levack, Hisashi Noma, Noyuri Yamaji, Erika Ota, Takeshi Hasegawa\",\"doi\":\"10.1186/s40560-025-00811-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prolonged mechanical ventilation is associated with an increased incidence of complications and higher mortality rates. Therefore, it is crucial to wean patients from mechanical ventilation as soon as possible. Recently, diaphragmatic ultrasound has been used in this decision-making process. This systematic review evaluated the effectiveness of diaphragmatic ultrasound to improve ventilator liberation outcomes.</p><p><strong>Methods: </strong>We searched three databases - MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. We included randomized control trials that compared the use of diaphragmatic ultrasound to standard care in adult patients on mechanical ventilation via tracheal intubation. We assessed risk of bias for included trials with the Cochrane Risk of Bias Tool and certainty of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation tool. For dichotomous outcomes, we reported risk ratios (RRs) with 95% confidence intervals (CIs). For continuous outcomes, we reported mean differences (MD) with 95% CIs if all retrieved records provide data on the same scale. The primary outcome was incidence of reintubation within 48 h of extubation and the secondary outcomes included duration of mechanical ventilation, incidence of reintubation rate after 48 h, ICU length of stay, and adverse events.</p><p><strong>Results: </strong>We found five relevant randomized controlled trials involving a total of 508 participants on mechanical ventilation in ICU following respiratory failure or surgery. Three studies (268 participants) provided data on the incidence of reintubation within 48 h of extubation. Using diaphragmatic ultrasound to guide extubation decisions led to a significant reduction in the risk of reintubation within 48 h (RR 0.62, 95% CI 0.41 to 0.95, low certainty of evidence). No significant differences were found in the duration of mechanical ventilation (MD - 1.39 h, 95% CI - 17.5 to 14.71 h, three studies, 268 participants, very low certainty of evidence) or reintubation after 48 h (RR 0.38, 95% CI 0.11-1.29, two studies, 240 participants, moderate certainty of evidence). However, ICU length of stay was significantly reduced in the diaphragmatic ultrasound group (MD - 1.0 days, 95% CI - 1.74 to - 0.26 days, one study, 130 participants, low certainty of evidence).</p><p><strong>Conclusion: </strong>Using diaphragmatic ultrasound in addition to standard clinical criteria to guide decisions around ventilator use and liberation resulted in a reduced risk of reintubation within 48 h of extubation when compared to standard clinical criteria alone.</p><p><strong>Systematic review registration: </strong>This systematic review was registered with the Open Science Framework: https://osf.io/cn8xf .</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"13 1\",\"pages\":\"40\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2025-07-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12288223/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-025-00811-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-025-00811-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
背景:延长机械通气与并发症发生率增加和死亡率升高有关。因此,尽快使患者脱离机械通气是至关重要的。最近,横膈膜超声已被用于这一决策过程。本系统综述评估了膈超声改善呼吸机解放效果的有效性。方法:我们检索了三个数据库:MEDLINE、Embase和Cochrane中央对照试验注册库。我们纳入了随机对照试验,比较了通过气管插管进行机械通气的成年患者使用膈超声和标准护理的情况。我们使用Cochrane偏倚风险工具评估纳入试验的偏倚风险,并使用分级推荐、评估、发展和评价工具评估证据的确定性。对于二分类结果,我们报告了95%置信区间(ci)的风险比(rr)。对于连续结果,如果所有检索记录提供相同尺度的数据,我们报告了95% ci的平均差异(MD)。主要结局为拔管后48 h内的再插管发生率,次要结局包括机械通气时间、48 h后再插管发生率、ICU住院时间和不良事件。结果:我们发现了5项相关的随机对照试验,共涉及508名受试者,在呼吸衰竭或手术后在ICU使用机械通气。三项研究(268名参与者)提供了拔管后48小时内再插管发生率的数据。使用膈超声指导拔管决定可显著降低48小时内再插管的风险(RR 0.62, 95% CI 0.41 ~ 0.95,证据确定性低)。机械通气持续时间(MD - 1.39 h, 95% CI - 17.5 - 14.71 h, 3项研究,268名受试者,证据确定性极低)或48小时后再插管(RR 0.38, 95% CI 0.11-1.29, 2项研究,240名受试者,证据确定性中等)无显著差异。然而,膈超声组的ICU住院时间明显缩短(MD - 1.0天,95% CI - 1.74至- 0.26天,一项研究,130名参与者,证据确定性低)。结论:与单独使用标准临床标准相比,使用膈肌超声指导呼吸机使用和释放的决定可降低拔管后48小时内重新插管的风险。系统综述注册:本系统综述注册于开放科学框架:https://osf.io/cn8xf。
Clinical utility of diaphragmatic ultrasound for mechanical ventilator liberation in adults: a systematic review and meta-analysis.
Background: Prolonged mechanical ventilation is associated with an increased incidence of complications and higher mortality rates. Therefore, it is crucial to wean patients from mechanical ventilation as soon as possible. Recently, diaphragmatic ultrasound has been used in this decision-making process. This systematic review evaluated the effectiveness of diaphragmatic ultrasound to improve ventilator liberation outcomes.
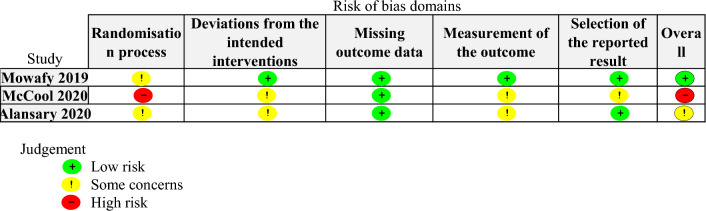
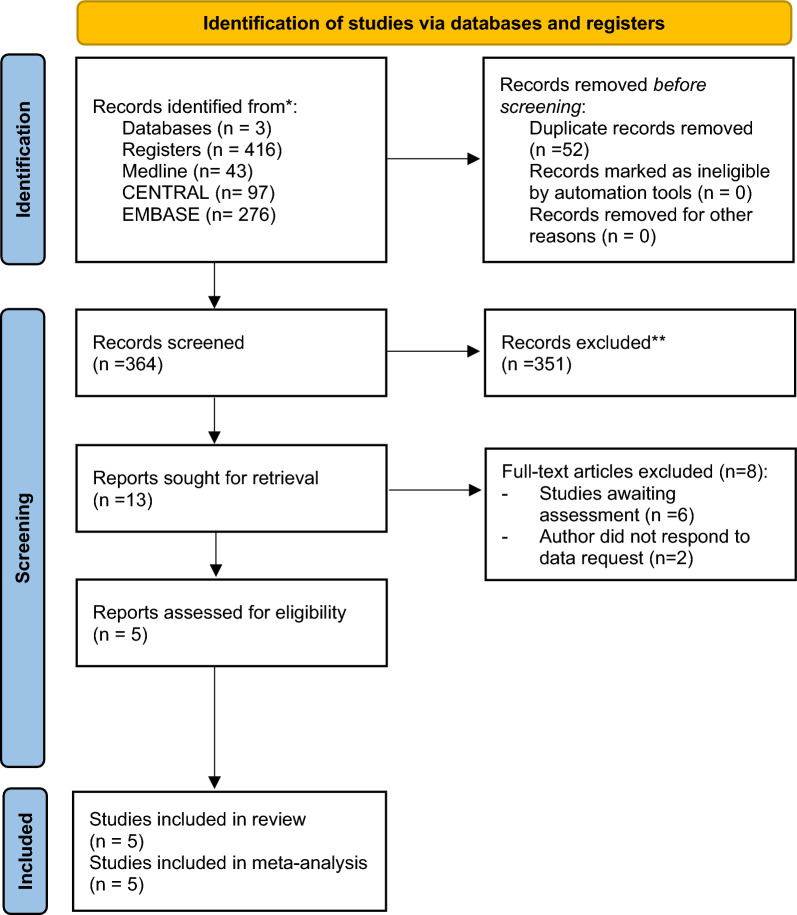
Methods: We searched three databases - MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials. We included randomized control trials that compared the use of diaphragmatic ultrasound to standard care in adult patients on mechanical ventilation via tracheal intubation. We assessed risk of bias for included trials with the Cochrane Risk of Bias Tool and certainty of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation tool. For dichotomous outcomes, we reported risk ratios (RRs) with 95% confidence intervals (CIs). For continuous outcomes, we reported mean differences (MD) with 95% CIs if all retrieved records provide data on the same scale. The primary outcome was incidence of reintubation within 48 h of extubation and the secondary outcomes included duration of mechanical ventilation, incidence of reintubation rate after 48 h, ICU length of stay, and adverse events.
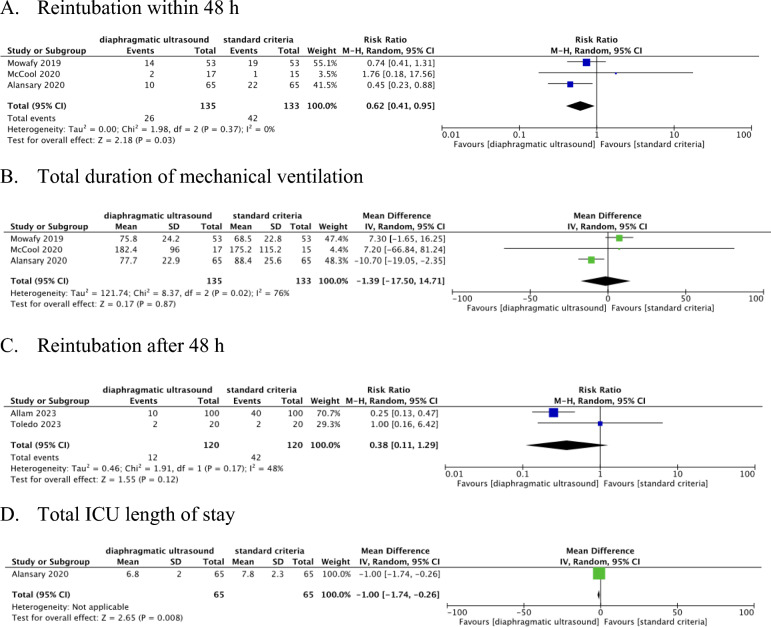
Results: We found five relevant randomized controlled trials involving a total of 508 participants on mechanical ventilation in ICU following respiratory failure or surgery. Three studies (268 participants) provided data on the incidence of reintubation within 48 h of extubation. Using diaphragmatic ultrasound to guide extubation decisions led to a significant reduction in the risk of reintubation within 48 h (RR 0.62, 95% CI 0.41 to 0.95, low certainty of evidence). No significant differences were found in the duration of mechanical ventilation (MD - 1.39 h, 95% CI - 17.5 to 14.71 h, three studies, 268 participants, very low certainty of evidence) or reintubation after 48 h (RR 0.38, 95% CI 0.11-1.29, two studies, 240 participants, moderate certainty of evidence). However, ICU length of stay was significantly reduced in the diaphragmatic ultrasound group (MD - 1.0 days, 95% CI - 1.74 to - 0.26 days, one study, 130 participants, low certainty of evidence).
Conclusion: Using diaphragmatic ultrasound in addition to standard clinical criteria to guide decisions around ventilator use and liberation resulted in a reduced risk of reintubation within 48 h of extubation when compared to standard clinical criteria alone.
Systematic review registration: This systematic review was registered with the Open Science Framework: https://osf.io/cn8xf .
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


