Xihua Zheng, Yumin Zhang, Huiying Huang, Ningbin Luo
{"title":"肝功能影像学评分预测肝细胞癌切除术后具有临床意义的PHLF。","authors":"Xihua Zheng, Yumin Zhang, Huiying Huang, Ningbin Luo","doi":"10.2147/JHC.S511240","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To develop a model based on Functional Liver Imaging Score (FLIS) to estimate the risk of clinically significant post-hepatectomy liver failure (PHLF) for hepatocellular carcinoma (HCC) after resection.</p><p><strong>Patients and methods: </strong>This retrospective study analyzed 885 patients with HCC who undergoing liver resection at our medical center between January 2017 and December 2021. Patients were randomly (7:3) assigned to development (n=620) or internal validation (n=265) cohorts. Univariable and multivariable logistic regression analyses were performed to identify independent risk factors for clinically significant PHLF, defined as grade B or C PHLF by the International Study Group of Liver Surgery. Predictive performance was assessed by the area under receiver operator characteristic curves (AUC).</p><p><strong>Results: </strong>Clinically significant PHLF occurred in 7.7% of the development cohort and 7.2% of the internal validation cohort. Multivariate analysis identified FLIS, major resection and ALBI score as independent predictors of clinically significant PHLF, and a model combining these three variables predicted failure in the development cohort (AUC 0.746, 95% CI 0.673-0.820) and internal validation cohort (AUC 0.717, 95% CI 0.595-0.838). The same model also predicted mortality within 90 days after surgery in the development cohort (AUC 0.704, 95% CI 0.575-0.832) and internal validation cohort (AUC 0.717, 95% CI 0.586-0.848). In both cohorts, overall survival rate was significantly lower among patients whom the model placed at high risk of clinically significant PHLF than among those at low risk.</p><p><strong>Conclusion: </strong>The combination of FLIS and other easily acquired clinical data may reliably predict clinically significant PHLF and mortality in hepatocellular carcinoma.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1483-1493"},"PeriodicalIF":3.4000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12283857/pdf/","citationCount":"0","resultStr":"{\"title\":\"Functional Liver Imaging Score to Predict Clinically Significant PHLF for Hepatocellular Carcinoma After Resection.\",\"authors\":\"Xihua Zheng, Yumin Zhang, Huiying Huang, Ningbin Luo\",\"doi\":\"10.2147/JHC.S511240\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To develop a model based on Functional Liver Imaging Score (FLIS) to estimate the risk of clinically significant post-hepatectomy liver failure (PHLF) for hepatocellular carcinoma (HCC) after resection.</p><p><strong>Patients and methods: </strong>This retrospective study analyzed 885 patients with HCC who undergoing liver resection at our medical center between January 2017 and December 2021. Patients were randomly (7:3) assigned to development (n=620) or internal validation (n=265) cohorts. Univariable and multivariable logistic regression analyses were performed to identify independent risk factors for clinically significant PHLF, defined as grade B or C PHLF by the International Study Group of Liver Surgery. Predictive performance was assessed by the area under receiver operator characteristic curves (AUC).</p><p><strong>Results: </strong>Clinically significant PHLF occurred in 7.7% of the development cohort and 7.2% of the internal validation cohort. Multivariate analysis identified FLIS, major resection and ALBI score as independent predictors of clinically significant PHLF, and a model combining these three variables predicted failure in the development cohort (AUC 0.746, 95% CI 0.673-0.820) and internal validation cohort (AUC 0.717, 95% CI 0.595-0.838). The same model also predicted mortality within 90 days after surgery in the development cohort (AUC 0.704, 95% CI 0.575-0.832) and internal validation cohort (AUC 0.717, 95% CI 0.586-0.848). In both cohorts, overall survival rate was significantly lower among patients whom the model placed at high risk of clinically significant PHLF than among those at low risk.</p><p><strong>Conclusion: </strong>The combination of FLIS and other easily acquired clinical data may reliably predict clinically significant PHLF and mortality in hepatocellular carcinoma.</p>\",\"PeriodicalId\":15906,\"journal\":{\"name\":\"Journal of Hepatocellular Carcinoma\",\"volume\":\"12 \",\"pages\":\"1483-1493\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12283857/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Hepatocellular Carcinoma\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/JHC.S511240\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S511240","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:建立基于肝功能影像学评分(FLIS)的模型,评估肝细胞癌(HCC)术后发生临床意义的肝切除术后肝功能衰竭(PHLF)的风险。患者和方法:本回顾性研究分析了2017年1月至2021年12月在我院行肝切除术的885例HCC患者。患者被随机(7:3)分配到发展(n=620)或内部验证(n=265)队列。进行单变量和多变量logistic回归分析,以确定临床显著性PHLF的独立危险因素,国际肝脏外科研究小组将PHLF定义为B级或C级。通过接收算子特征曲线下面积(AUC)评估预测性能。结果:有临床意义的PHLF发生率为7.7%的开发队列和7.2%的内部验证队列。多因素分析发现,FLIS、主要切除和ALBI评分是临床显著性PHLF的独立预测因素,结合这三个变量的模型预测了发展队列(AUC 0.746, 95% CI 0.673-0.820)和内部验证队列(AUC 0.717, 95% CI 0.595-0.838)的失败。该模型还预测了发展队列(AUC 0.704, 95% CI 0.575-0.832)和内部验证队列(AUC 0.717, 95% CI 0.586-0.848)术后90天内的死亡率。在这两个队列中,模型中处于临床显著性PHLF高风险的患者的总生存率明显低于低风险的患者。结论:结合FLIS和其他容易获得的临床数据,可以可靠地预测肝细胞癌的PHLF和死亡率。
Functional Liver Imaging Score to Predict Clinically Significant PHLF for Hepatocellular Carcinoma After Resection.
Purpose: To develop a model based on Functional Liver Imaging Score (FLIS) to estimate the risk of clinically significant post-hepatectomy liver failure (PHLF) for hepatocellular carcinoma (HCC) after resection.
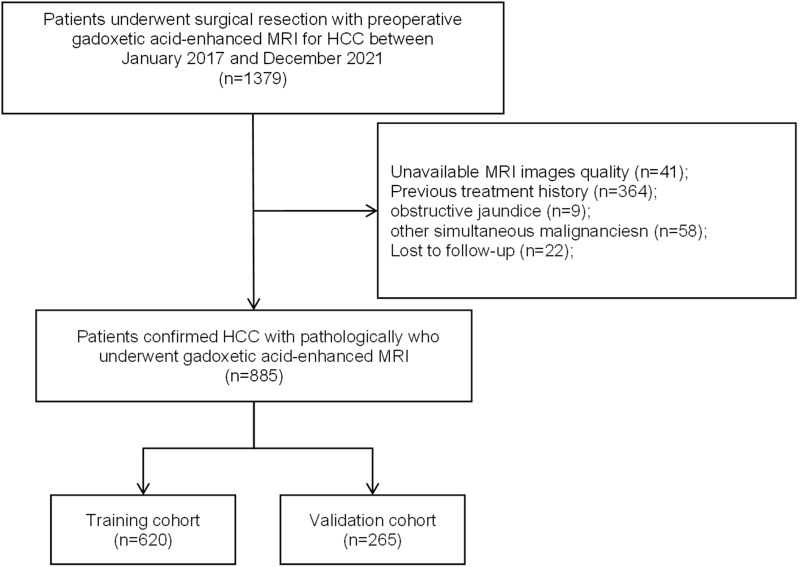
Patients and methods: This retrospective study analyzed 885 patients with HCC who undergoing liver resection at our medical center between January 2017 and December 2021. Patients were randomly (7:3) assigned to development (n=620) or internal validation (n=265) cohorts. Univariable and multivariable logistic regression analyses were performed to identify independent risk factors for clinically significant PHLF, defined as grade B or C PHLF by the International Study Group of Liver Surgery. Predictive performance was assessed by the area under receiver operator characteristic curves (AUC).
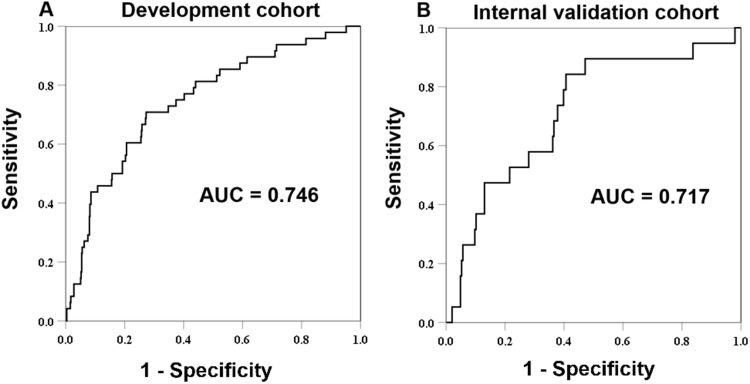
Results: Clinically significant PHLF occurred in 7.7% of the development cohort and 7.2% of the internal validation cohort. Multivariate analysis identified FLIS, major resection and ALBI score as independent predictors of clinically significant PHLF, and a model combining these three variables predicted failure in the development cohort (AUC 0.746, 95% CI 0.673-0.820) and internal validation cohort (AUC 0.717, 95% CI 0.595-0.838). The same model also predicted mortality within 90 days after surgery in the development cohort (AUC 0.704, 95% CI 0.575-0.832) and internal validation cohort (AUC 0.717, 95% CI 0.586-0.848). In both cohorts, overall survival rate was significantly lower among patients whom the model placed at high risk of clinically significant PHLF than among those at low risk.
Conclusion: The combination of FLIS and other easily acquired clinical data may reliably predict clinically significant PHLF and mortality in hepatocellular carcinoma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


