{"title":"病理生物学和转化科学对理解和管理缺血性心脏病的贡献:进展、障碍和未来方向。","authors":"L Maximilian Buja","doi":"10.145403/THIJ-25-8609","DOIUrl":null,"url":null,"abstract":"<p><p>Key pathobiological components of ischemic heart disease have been identified as follows: (1) In 1970 to 1973, myocardial infarct size was found to be the primary determinant of prognosis after acute myocardial infarction (AMI); (2) in 1973 to 1989, vulnerable coronary artery plaques were found to predispose individuals to coronary plaque disruption and thrombosis, causing major AMI; (3) in 1972, timely coronary reperfusion was demonstrated to limit the size of evolving AMI but with risk of reperfusion injury; and (4) in 1986, myocardial conditioning was found to be a clinically significant modulator capable of delaying AMI progression. Promising cardioprotective strategies combining timely reperfusion with conditioning in experimental animal and proof-of-concept human studies have not been shown to optimize cardioprotection, and this area of research has stalled. Nevertheless, opportunities for further progress against ischemic heart disease have come from new perspectives and approaches, including (1) recognition that functionally significant ischemic heart disease can result from microvascular dysfunction or epicardial coronary atherosclerosis; (2) rapid diagnosis of AMI subtypes through application of the Universal Definition of Myocardial Infarction based on high-sensitivity cardiac troponin measurements; (3) the Canadian Cardiovascular Society classification of AMI based on stages of tissue injury severity, as detected by advanced imaging; (4) implementation of the occlusion vs nonocclusion MI paradigm to prompt aggressive management of all ST-segment elevation MI and the one-third of non-ST-segment elevation MI with total occlusion; and (5) implementation of the Early Heart Attack Care program, which emphasizes prodromal symptom recognition to prevent AMI progression.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"52 2","pages":"e258609"},"PeriodicalIF":0.9000,"publicationDate":"2025-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277578/pdf/","citationCount":"0","resultStr":"{\"title\":\"Contributions of Pathobiological and Translational Science to Understanding and Managing Ischemic Heart Disease: Progress, Impediments, and Future Directions.\",\"authors\":\"L Maximilian Buja\",\"doi\":\"10.145403/THIJ-25-8609\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Key pathobiological components of ischemic heart disease have been identified as follows: (1) In 1970 to 1973, myocardial infarct size was found to be the primary determinant of prognosis after acute myocardial infarction (AMI); (2) in 1973 to 1989, vulnerable coronary artery plaques were found to predispose individuals to coronary plaque disruption and thrombosis, causing major AMI; (3) in 1972, timely coronary reperfusion was demonstrated to limit the size of evolving AMI but with risk of reperfusion injury; and (4) in 1986, myocardial conditioning was found to be a clinically significant modulator capable of delaying AMI progression. Promising cardioprotective strategies combining timely reperfusion with conditioning in experimental animal and proof-of-concept human studies have not been shown to optimize cardioprotection, and this area of research has stalled. Nevertheless, opportunities for further progress against ischemic heart disease have come from new perspectives and approaches, including (1) recognition that functionally significant ischemic heart disease can result from microvascular dysfunction or epicardial coronary atherosclerosis; (2) rapid diagnosis of AMI subtypes through application of the Universal Definition of Myocardial Infarction based on high-sensitivity cardiac troponin measurements; (3) the Canadian Cardiovascular Society classification of AMI based on stages of tissue injury severity, as detected by advanced imaging; (4) implementation of the occlusion vs nonocclusion MI paradigm to prompt aggressive management of all ST-segment elevation MI and the one-third of non-ST-segment elevation MI with total occlusion; and (5) implementation of the Early Heart Attack Care program, which emphasizes prodromal symptom recognition to prevent AMI progression.</p>\",\"PeriodicalId\":48680,\"journal\":{\"name\":\"Texas Heart Institute Journal\",\"volume\":\"52 2\",\"pages\":\"e258609\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-07-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12277578/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Texas Heart Institute Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.145403/THIJ-25-8609\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.145403/THIJ-25-8609","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Contributions of Pathobiological and Translational Science to Understanding and Managing Ischemic Heart Disease: Progress, Impediments, and Future Directions.
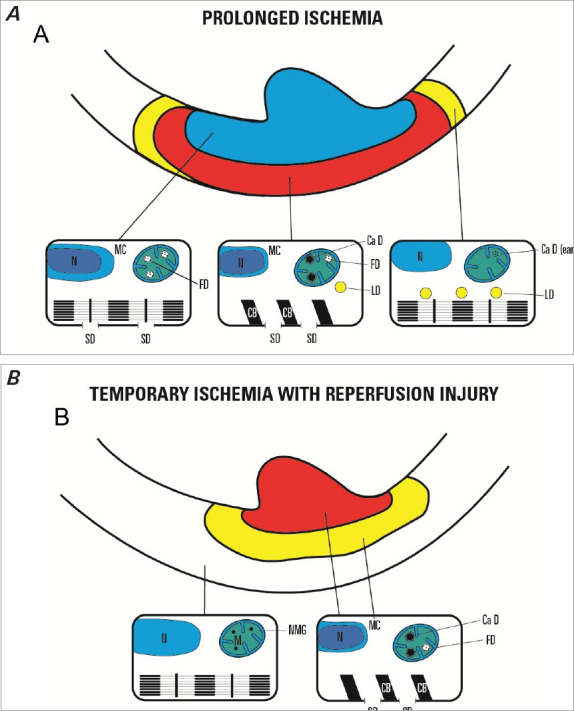
Key pathobiological components of ischemic heart disease have been identified as follows: (1) In 1970 to 1973, myocardial infarct size was found to be the primary determinant of prognosis after acute myocardial infarction (AMI); (2) in 1973 to 1989, vulnerable coronary artery plaques were found to predispose individuals to coronary plaque disruption and thrombosis, causing major AMI; (3) in 1972, timely coronary reperfusion was demonstrated to limit the size of evolving AMI but with risk of reperfusion injury; and (4) in 1986, myocardial conditioning was found to be a clinically significant modulator capable of delaying AMI progression. Promising cardioprotective strategies combining timely reperfusion with conditioning in experimental animal and proof-of-concept human studies have not been shown to optimize cardioprotection, and this area of research has stalled. Nevertheless, opportunities for further progress against ischemic heart disease have come from new perspectives and approaches, including (1) recognition that functionally significant ischemic heart disease can result from microvascular dysfunction or epicardial coronary atherosclerosis; (2) rapid diagnosis of AMI subtypes through application of the Universal Definition of Myocardial Infarction based on high-sensitivity cardiac troponin measurements; (3) the Canadian Cardiovascular Society classification of AMI based on stages of tissue injury severity, as detected by advanced imaging; (4) implementation of the occlusion vs nonocclusion MI paradigm to prompt aggressive management of all ST-segment elevation MI and the one-third of non-ST-segment elevation MI with total occlusion; and (5) implementation of the Early Heart Attack Care program, which emphasizes prodromal symptom recognition to prevent AMI progression.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


