Rahul Banerjee, Meera Mohan, Kai Rejeski, Benjamin R Puliafito, Diana D Cirstea, Gurbakhash Kaur, Shonali Midha, Georgia J McCaughan, Nikhil M Kumar, Nikita Mehra, Bhausaheb Bagal, Noopur S Raje
{"title":"对于多发性骨髓瘤,无论IgG水平如何,双特异性抗体治疗后应开始IVIG预防。","authors":"Rahul Banerjee, Meera Mohan, Kai Rejeski, Benjamin R Puliafito, Diana D Cirstea, Gurbakhash Kaur, Shonali Midha, Georgia J McCaughan, Nikhil M Kumar, Nikita Mehra, Bhausaheb Bagal, Noopur S Raje","doi":"10.1182/bloodadvances.2025016490","DOIUrl":null,"url":null,"abstract":"<p><strong>Abstract: </strong>Bispecific antibodies (bsAbs), such as teclistamab, elranatamab, linvoseltamab, and talquetamab, have impressive efficacy in multiple myeloma (MM) but come with substantial infectious risks that do not dissipate over time. Immunoglobulin replacement therapy (IgRT), which includes IV and subcutaneous (SC) immunoglobulins, may lower these risks. In this viewpoint, we contrast primary IgRT prophylaxis (initiation regardless of IgG levels) with preemptive IgRT treatment (initiation only once IgG levels fall below a certain threshold) in this setting. We make evidence-based arguments for primary prophylaxis as a safer and simpler approach than preemptive IgG-guided IgRT. We also discuss strategies to improve the cost-effectiveness of IV and SC immunoglobulins across the world. Given the overwhelmingly favorable benefit-risk profile of IgRT, coupled with the limitations inherent to IgG measurements in MM, withholding IgRT access based on arbitrary IgG thresholds is neither scientifically sound nor clinically appropriate for patients with MM who are receiving bsAb therapy.</p>","PeriodicalId":9228,"journal":{"name":"Blood advances","volume":" ","pages":"4720-4726"},"PeriodicalIF":7.1000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12466225/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immunoglobulin prophylaxis should be initiated after bispecific antibody therapy in multiple myeloma, regardless of IgG levels.\",\"authors\":\"Rahul Banerjee, Meera Mohan, Kai Rejeski, Benjamin R Puliafito, Diana D Cirstea, Gurbakhash Kaur, Shonali Midha, Georgia J McCaughan, Nikhil M Kumar, Nikita Mehra, Bhausaheb Bagal, Noopur S Raje\",\"doi\":\"10.1182/bloodadvances.2025016490\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Abstract: </strong>Bispecific antibodies (bsAbs), such as teclistamab, elranatamab, linvoseltamab, and talquetamab, have impressive efficacy in multiple myeloma (MM) but come with substantial infectious risks that do not dissipate over time. Immunoglobulin replacement therapy (IgRT), which includes IV and subcutaneous (SC) immunoglobulins, may lower these risks. In this viewpoint, we contrast primary IgRT prophylaxis (initiation regardless of IgG levels) with preemptive IgRT treatment (initiation only once IgG levels fall below a certain threshold) in this setting. We make evidence-based arguments for primary prophylaxis as a safer and simpler approach than preemptive IgG-guided IgRT. We also discuss strategies to improve the cost-effectiveness of IV and SC immunoglobulins across the world. Given the overwhelmingly favorable benefit-risk profile of IgRT, coupled with the limitations inherent to IgG measurements in MM, withholding IgRT access based on arbitrary IgG thresholds is neither scientifically sound nor clinically appropriate for patients with MM who are receiving bsAb therapy.</p>\",\"PeriodicalId\":9228,\"journal\":{\"name\":\"Blood advances\",\"volume\":\" \",\"pages\":\"4720-4726\"},\"PeriodicalIF\":7.1000,\"publicationDate\":\"2025-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12466225/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood advances\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1182/bloodadvances.2025016490\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood advances","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1182/bloodadvances.2025016490","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Immunoglobulin prophylaxis should be initiated after bispecific antibody therapy in multiple myeloma, regardless of IgG levels.
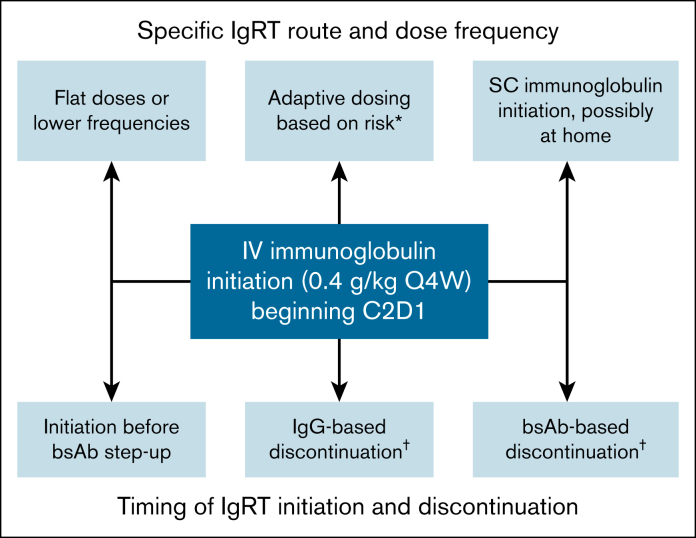
Abstract: Bispecific antibodies (bsAbs), such as teclistamab, elranatamab, linvoseltamab, and talquetamab, have impressive efficacy in multiple myeloma (MM) but come with substantial infectious risks that do not dissipate over time. Immunoglobulin replacement therapy (IgRT), which includes IV and subcutaneous (SC) immunoglobulins, may lower these risks. In this viewpoint, we contrast primary IgRT prophylaxis (initiation regardless of IgG levels) with preemptive IgRT treatment (initiation only once IgG levels fall below a certain threshold) in this setting. We make evidence-based arguments for primary prophylaxis as a safer and simpler approach than preemptive IgG-guided IgRT. We also discuss strategies to improve the cost-effectiveness of IV and SC immunoglobulins across the world. Given the overwhelmingly favorable benefit-risk profile of IgRT, coupled with the limitations inherent to IgG measurements in MM, withholding IgRT access based on arbitrary IgG thresholds is neither scientifically sound nor clinically appropriate for patients with MM who are receiving bsAb therapy.
期刊介绍:
Blood Advances, a semimonthly medical journal published by the American Society of Hematology, marks the first addition to the Blood family in 70 years. This peer-reviewed, online-only, open-access journal was launched under the leadership of founding editor-in-chief Robert Negrin, MD, from Stanford University Medical Center in Stanford, CA, with its inaugural issue released on November 29, 2016.
Blood Advances serves as an international platform for original articles detailing basic laboratory, translational, and clinical investigations in hematology. The journal comprehensively covers all aspects of hematology, including disorders of leukocytes (both benign and malignant), erythrocytes, platelets, hemostatic mechanisms, vascular biology, immunology, and hematologic oncology. Each article undergoes a rigorous peer-review process, with selection based on the originality of the findings, the high quality of the work presented, and the clarity of the presentation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


