Thais Faggion Vinholo, Andreas Habertheuer, Morgan Harloff, Sameer A. Hirji, Farhang Yazdchi, Siobhan McGurk, Borami Shin, Prem S. Shekar, Tsuyoshi Kaneko, Sary Aranki
{"title":"冠状动脉旁路移植术中无法钳夹主动脉的低温低流量纤颤:非体外循环冠状动脉搭桥术的替代方案","authors":"Thais Faggion Vinholo, Andreas Habertheuer, Morgan Harloff, Sameer A. Hirji, Farhang Yazdchi, Siobhan McGurk, Borami Shin, Prem S. Shekar, Tsuyoshi Kaneko, Sary Aranki","doi":"10.1155/jocs/1917682","DOIUrl":null,"url":null,"abstract":"<div>\n <p><b>Background:</b> Severe calcific disease of the ascending aorta may prohibit cross-clamping during coronary artery bypass grafting (CABG) due to unacceptable morbidity and mortality associated with atheroembolic complications. Clampless hypothermic noncardioplegic low flow fibrillation (HLFF) may minimize neurologic complications while allowing for complete revascularization.</p>\n <p><b>Methods:</b> From 2002 to 2019, 142 patients with unclampable aorta (UCA) underwent isolated CABG using clampless HLFF. Short-term and long-term outcomes were compared with an isolated conventional on-pump CABG cohort (<i>n</i> = 268) risk-matched (RM) for type of CABG, STS score, age, and sex.</p>\n <p><b>Results:</b> UCA and RM cohort patients were comparable in terms of age (73.7 ± 7.8 vs. 72.7 ± 8.7, <i>p</i> = 0.281), sex (34.4% vs. 32.5% female, <i>p</i> = 1.000), STS score (4.01 ± 3.43 vs. 3.80 ± 3.33, <i>p</i> = 0.539), and number of diseased vessels (<i>p</i> = 0.323). 90% of patients underwent central cannulation; UCA group patients received a comparable number of arterial (<i>p</i> = 0.432) or venous grafts (<i>p</i> = 0.493). Incidence of stroke was 6.3% in the UCA cohort and 2.6% in the RM cohort (<i>p</i> = 0.059). Need for reoperation, postoperative transfusions, incidence of atrial fibrillation, and renal impairment was similar (all <i>p</i> > 0.050). UCA patients spent a longer time on the ventilator, in the ICU, and in the hospital (all <i>p</i> = 0.001). Operative mortality was not different between UCA and RM groups (3.5% vs. 4.5%, <i>p</i> = 0.797) as was all-cause mortality over long-term follow-up (<i>p</i> = 0.093).</p>\n <p><b>Conclusions:</b> While a higher incidence of stroke was observed, without reaching statistical significance, hypothermic fibrillatory arrest remains a valuable and safe tool for coronary revascularization in UCA patients, offering comparable short-term and long-term survival outcomes allowing for complete revascularization.</p>\n </div>","PeriodicalId":15367,"journal":{"name":"Journal of Cardiac Surgery","volume":"2025 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2025-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/jocs/1917682","citationCount":"0","resultStr":"{\"title\":\"Hypothermic Low Flow Fibrillation for Unclampable Aorta in Coronary Artery Bypass Grafting: Alternative to Off-Pump CABG\",\"authors\":\"Thais Faggion Vinholo, Andreas Habertheuer, Morgan Harloff, Sameer A. Hirji, Farhang Yazdchi, Siobhan McGurk, Borami Shin, Prem S. Shekar, Tsuyoshi Kaneko, Sary Aranki\",\"doi\":\"10.1155/jocs/1917682\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n <p><b>Background:</b> Severe calcific disease of the ascending aorta may prohibit cross-clamping during coronary artery bypass grafting (CABG) due to unacceptable morbidity and mortality associated with atheroembolic complications. Clampless hypothermic noncardioplegic low flow fibrillation (HLFF) may minimize neurologic complications while allowing for complete revascularization.</p>\\n <p><b>Methods:</b> From 2002 to 2019, 142 patients with unclampable aorta (UCA) underwent isolated CABG using clampless HLFF. Short-term and long-term outcomes were compared with an isolated conventional on-pump CABG cohort (<i>n</i> = 268) risk-matched (RM) for type of CABG, STS score, age, and sex.</p>\\n <p><b>Results:</b> UCA and RM cohort patients were comparable in terms of age (73.7 ± 7.8 vs. 72.7 ± 8.7, <i>p</i> = 0.281), sex (34.4% vs. 32.5% female, <i>p</i> = 1.000), STS score (4.01 ± 3.43 vs. 3.80 ± 3.33, <i>p</i> = 0.539), and number of diseased vessels (<i>p</i> = 0.323). 90% of patients underwent central cannulation; UCA group patients received a comparable number of arterial (<i>p</i> = 0.432) or venous grafts (<i>p</i> = 0.493). Incidence of stroke was 6.3% in the UCA cohort and 2.6% in the RM cohort (<i>p</i> = 0.059). Need for reoperation, postoperative transfusions, incidence of atrial fibrillation, and renal impairment was similar (all <i>p</i> > 0.050). UCA patients spent a longer time on the ventilator, in the ICU, and in the hospital (all <i>p</i> = 0.001). Operative mortality was not different between UCA and RM groups (3.5% vs. 4.5%, <i>p</i> = 0.797) as was all-cause mortality over long-term follow-up (<i>p</i> = 0.093).</p>\\n <p><b>Conclusions:</b> While a higher incidence of stroke was observed, without reaching statistical significance, hypothermic fibrillatory arrest remains a valuable and safe tool for coronary revascularization in UCA patients, offering comparable short-term and long-term survival outcomes allowing for complete revascularization.</p>\\n </div>\",\"PeriodicalId\":15367,\"journal\":{\"name\":\"Journal of Cardiac Surgery\",\"volume\":\"2025 1\",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-07-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1155/jocs/1917682\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiac Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1155/jocs/1917682\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiac Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/jocs/1917682","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Hypothermic Low Flow Fibrillation for Unclampable Aorta in Coronary Artery Bypass Grafting: Alternative to Off-Pump CABG
Background: Severe calcific disease of the ascending aorta may prohibit cross-clamping during coronary artery bypass grafting (CABG) due to unacceptable morbidity and mortality associated with atheroembolic complications. Clampless hypothermic noncardioplegic low flow fibrillation (HLFF) may minimize neurologic complications while allowing for complete revascularization.
Methods: From 2002 to 2019, 142 patients with unclampable aorta (UCA) underwent isolated CABG using clampless HLFF. Short-term and long-term outcomes were compared with an isolated conventional on-pump CABG cohort (n = 268) risk-matched (RM) for type of CABG, STS score, age, and sex.
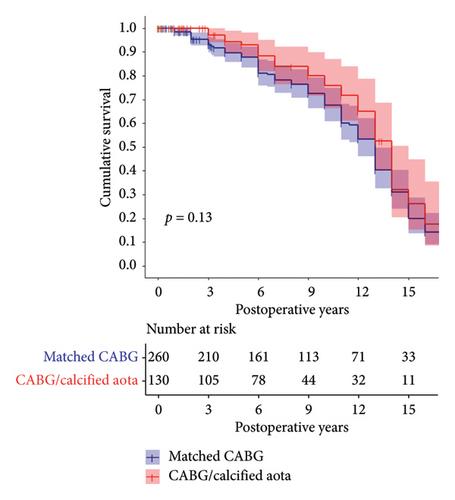
Results: UCA and RM cohort patients were comparable in terms of age (73.7 ± 7.8 vs. 72.7 ± 8.7, p = 0.281), sex (34.4% vs. 32.5% female, p = 1.000), STS score (4.01 ± 3.43 vs. 3.80 ± 3.33, p = 0.539), and number of diseased vessels (p = 0.323). 90% of patients underwent central cannulation; UCA group patients received a comparable number of arterial (p = 0.432) or venous grafts (p = 0.493). Incidence of stroke was 6.3% in the UCA cohort and 2.6% in the RM cohort (p = 0.059). Need for reoperation, postoperative transfusions, incidence of atrial fibrillation, and renal impairment was similar (all p > 0.050). UCA patients spent a longer time on the ventilator, in the ICU, and in the hospital (all p = 0.001). Operative mortality was not different between UCA and RM groups (3.5% vs. 4.5%, p = 0.797) as was all-cause mortality over long-term follow-up (p = 0.093).
Conclusions: While a higher incidence of stroke was observed, without reaching statistical significance, hypothermic fibrillatory arrest remains a valuable and safe tool for coronary revascularization in UCA patients, offering comparable short-term and long-term survival outcomes allowing for complete revascularization.
期刊介绍:
Journal of Cardiac Surgery (JCS) is a peer-reviewed journal devoted to contemporary surgical treatment of cardiac disease. Renown for its detailed "how to" methods, JCS''s well-illustrated, concise technical articles, critical reviews and commentaries are highly valued by dedicated readers worldwide.
With Editor-in-Chief Harold Lazar, MD and an internationally prominent editorial board, JCS continues its 20-year history as an important professional resource. Editorial coverage includes biologic support, mechanical cardiac assist and/or replacement and surgical techniques, and features current material on topics such as OPCAB surgery, stented and stentless valves, endovascular stent placement, atrial fibrillation, transplantation, percutaneous valve repair/replacement, left ventricular restoration surgery, immunobiology, and bridges to transplant and recovery.
In addition, special sections (Images in Cardiac Surgery, Cardiac Regeneration) and historical reviews stimulate reader interest. The journal also routinely publishes proceedings of important international symposia in a timely manner.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


