Khalid A Ishani, Anders Westanmo, Amy Gravely, Meredith C McCormack, Arianne K Baldomero
{"title":"导航医疗保健中的数据可用性挑战:评估肺功能测试对死亡率风险的护理评估需求评分的附加价值","authors":"Khalid A Ishani, Anders Westanmo, Amy Gravely, Meredith C McCormack, Arianne K Baldomero","doi":"10.1136/bmjhci-2024-101361","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Pulmonary function testing (PFT) data, such as forced expiratory volume (FEV<sub>1</sub>) has become increasingly siloed from the electronic health record (EHR). We hypothesised that FEV<sub>1</sub> %pred is independently associated with mortality risk, even after adjusting for the Care Assessment Needs (CAN) score, a validated method developed by the Veterans Health Administration (VA) to predict mortality. Additionally, we hypothesised that the integration of PFT data into the EHR has declined in recent years.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study using national VA data on PFTs from 2013 to 2018. Using logistic regression adjusted for CAN scores, we assessed the associations between FEV1 percent predicted (%pred) and all-cause mortality at 1 year and 5 years.</p><p><strong>Results: </strong>While the number of PFTs performed has generally increased since 2000, the integration of PFT data into the EHR has declined since 2006. The CAN-adjusted odds of 1-year mortality were 2.94 (95% CI: 2.66 to 3.24) for those with FEV<sub>1</sub> %pred <35%, compared with those with FEV<sub>1</sub> %pred ≥70%, while 5-year mortality odds were 3.83 (95% CI: 3.58 to 4.09).</p><p><strong>Discussion: </strong>Our study shows that FEV<sub>1</sub> %pred is statistically significantly associated with increased risk of mortality, above and beyond the CAN score. However, the declining integration of PFT data into the VA EHR highlights a concerning trend of isolating critical test results from clinical care.</p><p><strong>Conclusion: </strong>Among people with FEV<sub>1</sub> recorded in the EHR, FEV<sub>1</sub> %pred is statistically significantly associated with increased risk of both 1-year and 5-year mortality, above and beyond the CAN score.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"32 1","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2025-07-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278127/pdf/","citationCount":"0","resultStr":"{\"title\":\"Navigating data availability challenges in healthcare: assessing the added value of pulmonary function testing to the Care Assessment Need score for mortality risk.\",\"authors\":\"Khalid A Ishani, Anders Westanmo, Amy Gravely, Meredith C McCormack, Arianne K Baldomero\",\"doi\":\"10.1136/bmjhci-2024-101361\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Pulmonary function testing (PFT) data, such as forced expiratory volume (FEV<sub>1</sub>) has become increasingly siloed from the electronic health record (EHR). We hypothesised that FEV<sub>1</sub> %pred is independently associated with mortality risk, even after adjusting for the Care Assessment Needs (CAN) score, a validated method developed by the Veterans Health Administration (VA) to predict mortality. Additionally, we hypothesised that the integration of PFT data into the EHR has declined in recent years.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study using national VA data on PFTs from 2013 to 2018. Using logistic regression adjusted for CAN scores, we assessed the associations between FEV1 percent predicted (%pred) and all-cause mortality at 1 year and 5 years.</p><p><strong>Results: </strong>While the number of PFTs performed has generally increased since 2000, the integration of PFT data into the EHR has declined since 2006. The CAN-adjusted odds of 1-year mortality were 2.94 (95% CI: 2.66 to 3.24) for those with FEV<sub>1</sub> %pred <35%, compared with those with FEV<sub>1</sub> %pred ≥70%, while 5-year mortality odds were 3.83 (95% CI: 3.58 to 4.09).</p><p><strong>Discussion: </strong>Our study shows that FEV<sub>1</sub> %pred is statistically significantly associated with increased risk of mortality, above and beyond the CAN score. However, the declining integration of PFT data into the VA EHR highlights a concerning trend of isolating critical test results from clinical care.</p><p><strong>Conclusion: </strong>Among people with FEV<sub>1</sub> recorded in the EHR, FEV<sub>1</sub> %pred is statistically significantly associated with increased risk of both 1-year and 5-year mortality, above and beyond the CAN score.</p>\",\"PeriodicalId\":9050,\"journal\":{\"name\":\"BMJ Health & Care Informatics\",\"volume\":\"32 1\",\"pages\":\"\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-07-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12278127/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Health & Care Informatics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjhci-2024-101361\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2024-101361","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Navigating data availability challenges in healthcare: assessing the added value of pulmonary function testing to the Care Assessment Need score for mortality risk.
Objectives: Pulmonary function testing (PFT) data, such as forced expiratory volume (FEV1) has become increasingly siloed from the electronic health record (EHR). We hypothesised that FEV1 %pred is independently associated with mortality risk, even after adjusting for the Care Assessment Needs (CAN) score, a validated method developed by the Veterans Health Administration (VA) to predict mortality. Additionally, we hypothesised that the integration of PFT data into the EHR has declined in recent years.
Methods: We conducted a retrospective cohort study using national VA data on PFTs from 2013 to 2018. Using logistic regression adjusted for CAN scores, we assessed the associations between FEV1 percent predicted (%pred) and all-cause mortality at 1 year and 5 years.
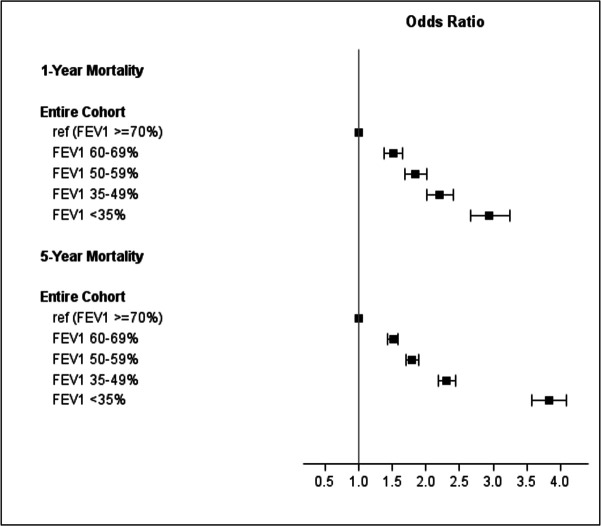
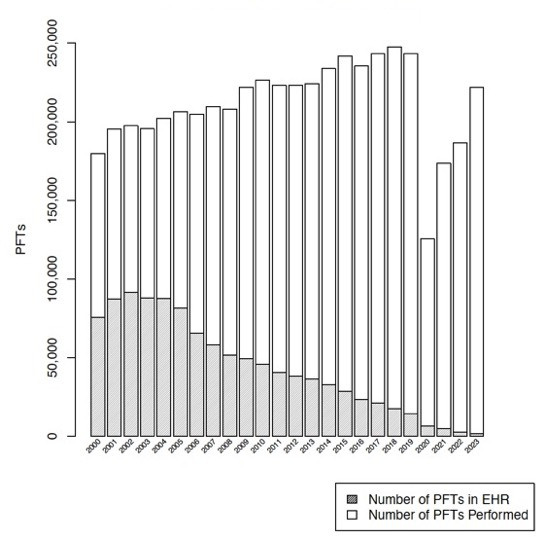
Results: While the number of PFTs performed has generally increased since 2000, the integration of PFT data into the EHR has declined since 2006. The CAN-adjusted odds of 1-year mortality were 2.94 (95% CI: 2.66 to 3.24) for those with FEV1 %pred <35%, compared with those with FEV1 %pred ≥70%, while 5-year mortality odds were 3.83 (95% CI: 3.58 to 4.09).
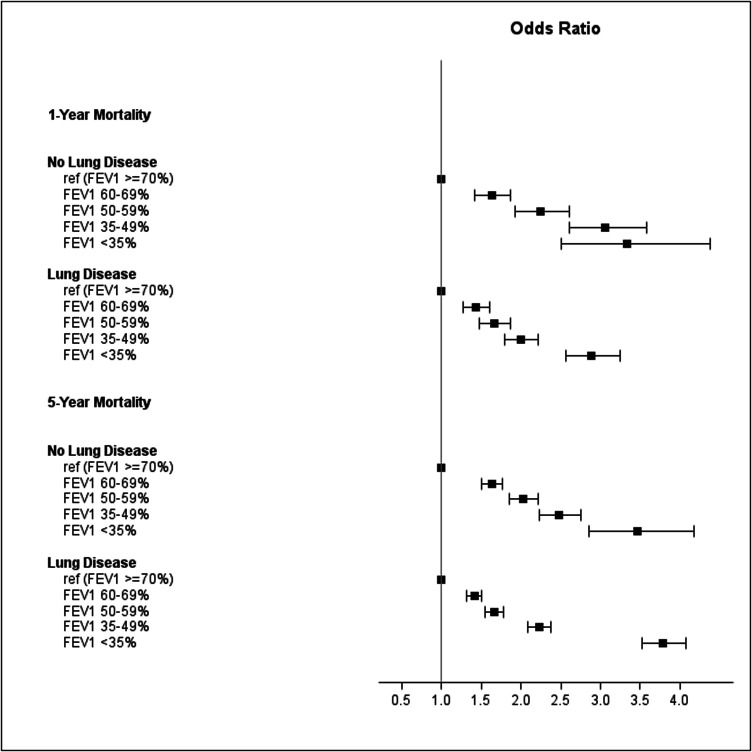
Discussion: Our study shows that FEV1 %pred is statistically significantly associated with increased risk of mortality, above and beyond the CAN score. However, the declining integration of PFT data into the VA EHR highlights a concerning trend of isolating critical test results from clinical care.
Conclusion: Among people with FEV1 recorded in the EHR, FEV1 %pred is statistically significantly associated with increased risk of both 1-year and 5-year mortality, above and beyond the CAN score.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


