Ibrahim Alfayoumi, Asmita Priyadarshini Khatiwada, Surachat Ngorsuraches
{"title":"在美国,托利帕单抗联合阿西替尼治疗晚期肾细胞癌患者的成本-效果分析。","authors":"Ibrahim Alfayoumi, Asmita Priyadarshini Khatiwada, Surachat Ngorsuraches","doi":"10.1007/s40261-025-01464-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The RENOTORCH trial found that toripalimab plus axitinib extended progression-free and overall survival in patients with advanced renal cell carcinoma (RCC), though its financial burden may limit widespread use. This study aimed to assess the cost-effectiveness of toripalimab plus axitinib compared with sunitinib monotherapy as a first-line therapy for patients with previously untreated or intermediate- or poor-risk advanced RCC from a US third-party payer perspective.</p><p><strong>Methods: </strong>A three-state partitioned survival model (progression-free, progression, death) was utilized, with clinical outcomes obtained from the RENOTORCH trial. Progression-free survival (PFS) and overall survival (OS) were modeled using various parametric functions over a 5-year horizon, applying a 3% annual discount rate. Costs of treatments, administration, monitoring, and management of grade 3/4 adverse events (≥ 5% occurrence) were sourced from Micromedex® and Centers for Medicare & Medicaid Services (CMS) databases. Life years (LY), quality-adjusted life years (QALY), and incremental costs per LY and QALY were estimated. One-way and probabilistic sensitivity analyses were conducted. Subgroup analyses for intermediate- and poor-risk patients, as classified by the International Metastatic RCC Database Consortium (IMDC) criteria, were performed using similar methods.</p><p><strong>Results: </strong>Toripalimab plus axitinib increased total costs by $332,359, gained 0.68 LY and 0.36 QALY compared with sunitinib, resulting in incremental costs of $489,747 per LY and $923,962 per QALY. One-way sensitivity analysis showed that the incremental cost per QALY was most sensitive to changes in toripalimab plus axitinib's cost. At a $150,000 willingness-to-pay threshold, probabilistic sensitivity analysis showed a nearly 0% probability of toripalimab plus axitinib being cost-effective. Similarly, toripalimab plus axitinib was still not cost-effective for intermediate- and poor-risk patients.</p><p><strong>Conclusions: </strong>Compared with sunitinib monotherapy, our study suggested that toripalimab plus axitinib was not cost-effective for patients with advanced renal cell carcinoma from a US third-party payer perspective. Further analyses are warranted when more data are available. Despite benefits across different risk groups, toripalimab plus axitinib was not cost-effective for intermediate- and poor-risk patients.</p>","PeriodicalId":10402,"journal":{"name":"Clinical Drug Investigation","volume":" ","pages":"537-549"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12307552/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-Effectiveness Analysis of Toripalimab Plus Axitinib for Patients with Advanced Renal Cell Carcinoma in the United States.\",\"authors\":\"Ibrahim Alfayoumi, Asmita Priyadarshini Khatiwada, Surachat Ngorsuraches\",\"doi\":\"10.1007/s40261-025-01464-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The RENOTORCH trial found that toripalimab plus axitinib extended progression-free and overall survival in patients with advanced renal cell carcinoma (RCC), though its financial burden may limit widespread use. This study aimed to assess the cost-effectiveness of toripalimab plus axitinib compared with sunitinib monotherapy as a first-line therapy for patients with previously untreated or intermediate- or poor-risk advanced RCC from a US third-party payer perspective.</p><p><strong>Methods: </strong>A three-state partitioned survival model (progression-free, progression, death) was utilized, with clinical outcomes obtained from the RENOTORCH trial. Progression-free survival (PFS) and overall survival (OS) were modeled using various parametric functions over a 5-year horizon, applying a 3% annual discount rate. Costs of treatments, administration, monitoring, and management of grade 3/4 adverse events (≥ 5% occurrence) were sourced from Micromedex® and Centers for Medicare & Medicaid Services (CMS) databases. Life years (LY), quality-adjusted life years (QALY), and incremental costs per LY and QALY were estimated. One-way and probabilistic sensitivity analyses were conducted. Subgroup analyses for intermediate- and poor-risk patients, as classified by the International Metastatic RCC Database Consortium (IMDC) criteria, were performed using similar methods.</p><p><strong>Results: </strong>Toripalimab plus axitinib increased total costs by $332,359, gained 0.68 LY and 0.36 QALY compared with sunitinib, resulting in incremental costs of $489,747 per LY and $923,962 per QALY. One-way sensitivity analysis showed that the incremental cost per QALY was most sensitive to changes in toripalimab plus axitinib's cost. At a $150,000 willingness-to-pay threshold, probabilistic sensitivity analysis showed a nearly 0% probability of toripalimab plus axitinib being cost-effective. Similarly, toripalimab plus axitinib was still not cost-effective for intermediate- and poor-risk patients.</p><p><strong>Conclusions: </strong>Compared with sunitinib monotherapy, our study suggested that toripalimab plus axitinib was not cost-effective for patients with advanced renal cell carcinoma from a US third-party payer perspective. Further analyses are warranted when more data are available. Despite benefits across different risk groups, toripalimab plus axitinib was not cost-effective for intermediate- and poor-risk patients.</p>\",\"PeriodicalId\":10402,\"journal\":{\"name\":\"Clinical Drug Investigation\",\"volume\":\" \",\"pages\":\"537-549\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12307552/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Drug Investigation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40261-025-01464-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Drug Investigation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40261-025-01464-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Cost-Effectiveness Analysis of Toripalimab Plus Axitinib for Patients with Advanced Renal Cell Carcinoma in the United States.
Objective: The RENOTORCH trial found that toripalimab plus axitinib extended progression-free and overall survival in patients with advanced renal cell carcinoma (RCC), though its financial burden may limit widespread use. This study aimed to assess the cost-effectiveness of toripalimab plus axitinib compared with sunitinib monotherapy as a first-line therapy for patients with previously untreated or intermediate- or poor-risk advanced RCC from a US third-party payer perspective.
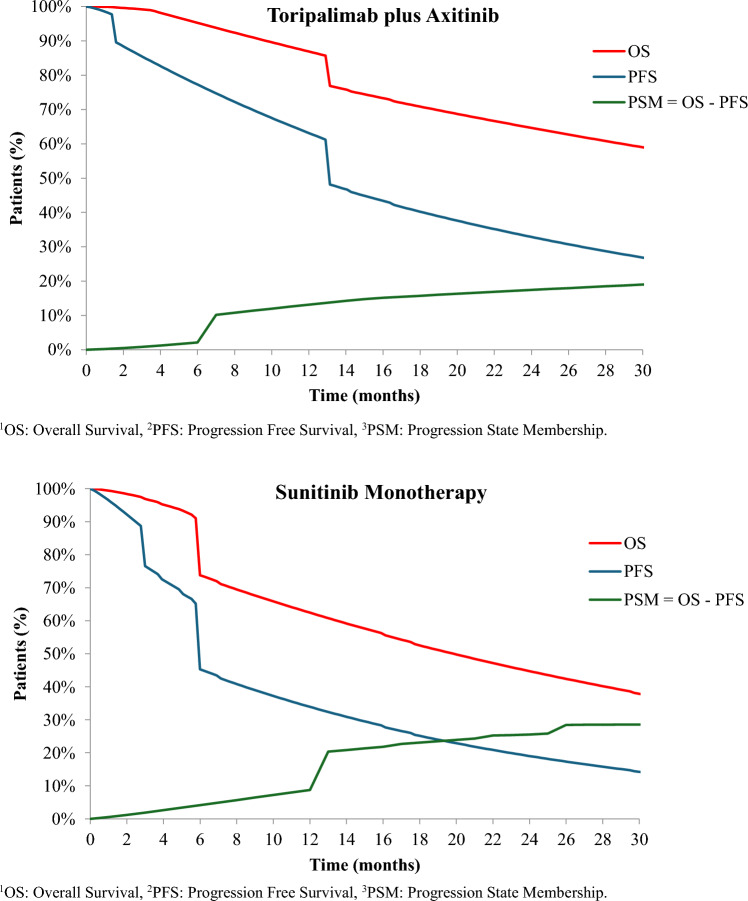
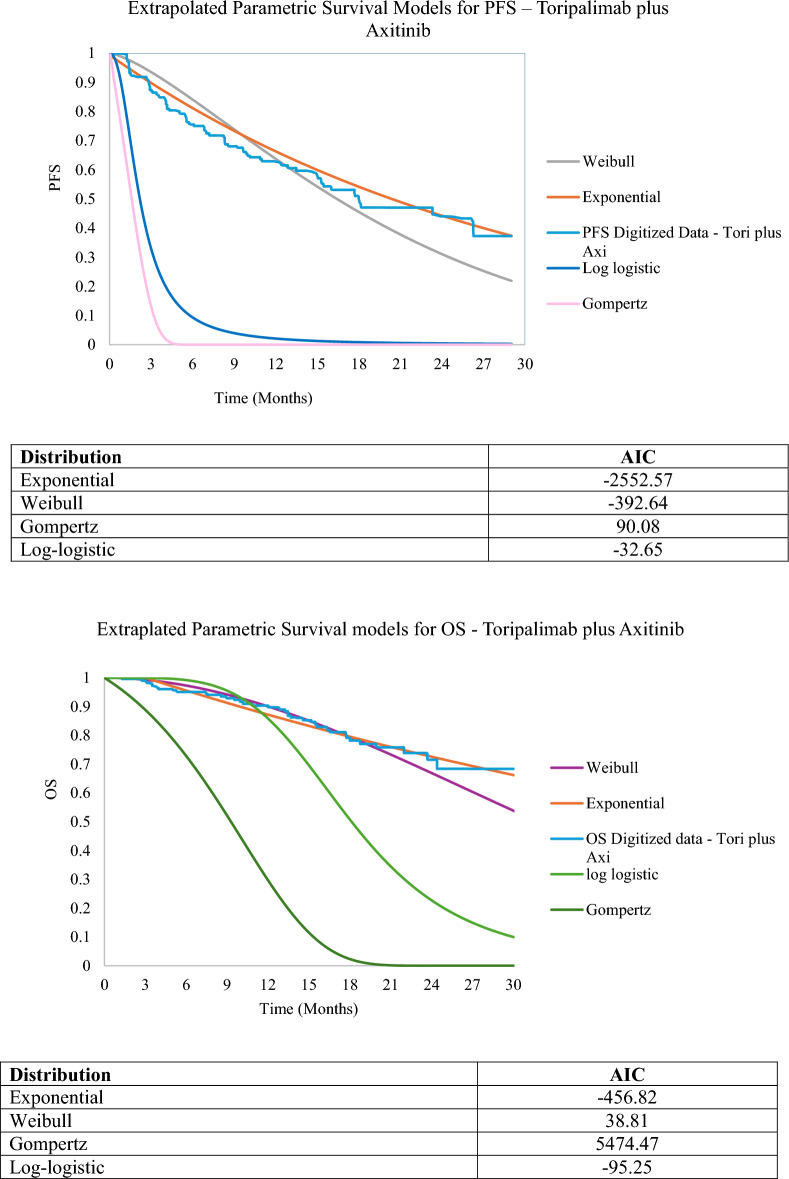
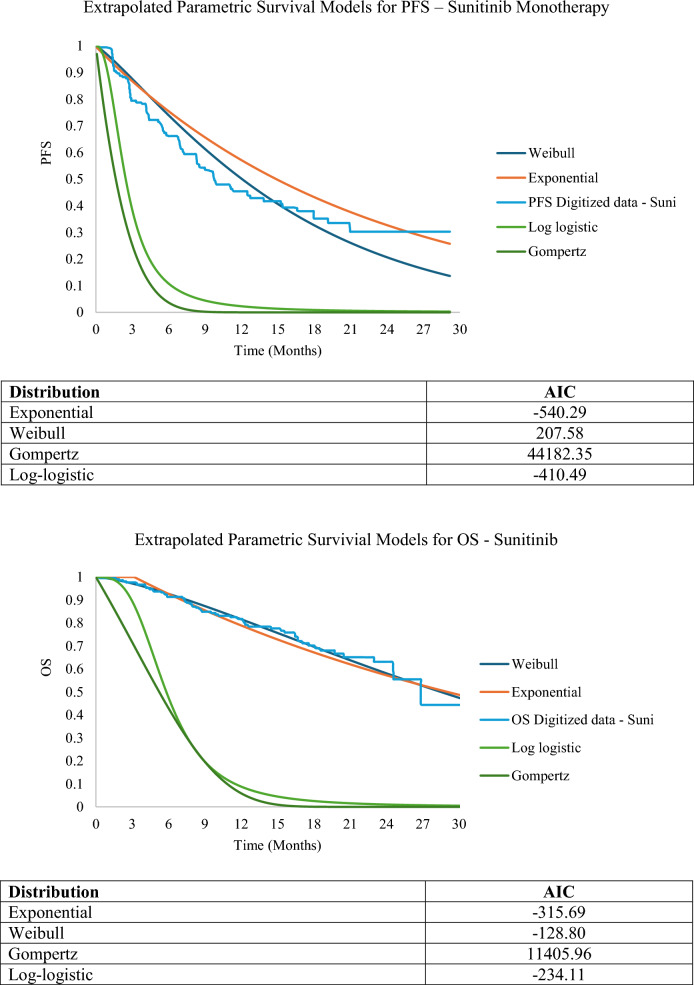
Methods: A three-state partitioned survival model (progression-free, progression, death) was utilized, with clinical outcomes obtained from the RENOTORCH trial. Progression-free survival (PFS) and overall survival (OS) were modeled using various parametric functions over a 5-year horizon, applying a 3% annual discount rate. Costs of treatments, administration, monitoring, and management of grade 3/4 adverse events (≥ 5% occurrence) were sourced from Micromedex® and Centers for Medicare & Medicaid Services (CMS) databases. Life years (LY), quality-adjusted life years (QALY), and incremental costs per LY and QALY were estimated. One-way and probabilistic sensitivity analyses were conducted. Subgroup analyses for intermediate- and poor-risk patients, as classified by the International Metastatic RCC Database Consortium (IMDC) criteria, were performed using similar methods.
Results: Toripalimab plus axitinib increased total costs by $332,359, gained 0.68 LY and 0.36 QALY compared with sunitinib, resulting in incremental costs of $489,747 per LY and $923,962 per QALY. One-way sensitivity analysis showed that the incremental cost per QALY was most sensitive to changes in toripalimab plus axitinib's cost. At a $150,000 willingness-to-pay threshold, probabilistic sensitivity analysis showed a nearly 0% probability of toripalimab plus axitinib being cost-effective. Similarly, toripalimab plus axitinib was still not cost-effective for intermediate- and poor-risk patients.
Conclusions: Compared with sunitinib monotherapy, our study suggested that toripalimab plus axitinib was not cost-effective for patients with advanced renal cell carcinoma from a US third-party payer perspective. Further analyses are warranted when more data are available. Despite benefits across different risk groups, toripalimab plus axitinib was not cost-effective for intermediate- and poor-risk patients.
期刊介绍:
Clinical Drug Investigation provides rapid publication of original research covering all phases of clinical drug development and therapeutic use of drugs. The Journal includes:
-Clinical trials, outcomes research, clinical pharmacoeconomic studies and pharmacoepidemiology studies with a strong link to optimum prescribing practice for a drug or group of drugs.
-Clinical pharmacodynamic and clinical pharmacokinetic studies with a strong link to clinical practice.
-Pharmacodynamic and pharmacokinetic studies in healthy volunteers in which significant implications for clinical prescribing are discussed.
-Studies focusing on the application of drug delivery technology in healthcare.
-Short communications and case study reports that meet the above criteria will also be considered.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Clinical Drug Investigation may be accompanied by plain language summaries to assist readers who have some knowledge, but non in-depth expertise in, the area to understand important medical advances.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


