{"title":"老年脑血管疾病患者死前认知轨迹与a β和tau生物标志物相关:一项纵向队列研究","authors":"Emily Rosenich, Yen Ying Lim","doi":"10.1186/s13195-025-01776-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Beta-amyloid (Aβ) plaques and tau tangles are pathological hallmarks of Alzheimer's disease (AD); however, autopsy studies reveal that most older adults also present with cerebrovascular disease (CVD) markers. It remains unclear how Aβ and tau relate to cognition in the context of concurrent CVD. In initially cognitively unimpaired older adults with CVD, this study aimed to determine ante-mortem cognitive trajectories associated with elevated Aβ and/or tau at autopsy.</p><p><strong>Methods: </strong>Participants aged 65-95 classified as cognitively unimpaired at baseline from the National Alzheimer's Coordinating Center database, with ≥ 1 follow-up between 2005 and 2015, and available autopsy/APOE data were included in this cohort study (N = 863). All participants had at least one of six CVD markers at autopsy. Participants were classified into four groups (A - T-, A + T-, A - T+, A + T+) based on semiquantitative Consortium to Establish a Registry for Alzheimer's Disease neuritic plaque staging and Braak staging. Linear mixed models assessed rate of change in Preclinical Alzheimer's Cognitive Composite scores, episodic memory, and executive function.</p><p><strong>Results: </strong>A + T + adults demonstrated significantly faster cognitive decline on all outcomes in the ~ 10 years preceding death compared to A - T- adults (d = 0.34-0.46). Similarly, when compared to A + T - adults, A + T + adults showed significantly faster decline on all outcomes (d = 0.19-0.37). At the last visit prior to death, a greater proportion of A + T + adults (36%) received a dementia diagnosis compared to A - T+ (15%; OR = 6.00), A + T- (14%; OR = 8.00) and A - T- adults (12%; OR = 6.86), p <.001. When analyses were restricted to exclude dementia diagnoses, significantly faster decline on all outcomes (p's < 0.001, d = 0.29-0.37) was similarly observed in A + T + adults compared to A - T- adults.</p><p><strong>Conclusions: </strong>In older adults with concurrent CVD, A + T + at autopsy was associated with greater cognitive decline over 10 years preceding death compared to A - T- older adults. Faster cognitive decline in A + T + in the context of low final visit dementia diagnoses may suggest that post-mortem A + T + is associated with a steep trajectory of cognitive decline ante-mortem, but that dementia progression is not inevitable.</p>","PeriodicalId":7516,"journal":{"name":"Alzheimer's Research & Therapy","volume":"17 1","pages":"165"},"PeriodicalIF":7.6000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12273324/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ante-mortem cognitive trajectories associated with Aβ and tau biomarker profiles in older adults with cerebrovascular disease: a longitudinal cohort study.\",\"authors\":\"Emily Rosenich, Yen Ying Lim\",\"doi\":\"10.1186/s13195-025-01776-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Beta-amyloid (Aβ) plaques and tau tangles are pathological hallmarks of Alzheimer's disease (AD); however, autopsy studies reveal that most older adults also present with cerebrovascular disease (CVD) markers. It remains unclear how Aβ and tau relate to cognition in the context of concurrent CVD. In initially cognitively unimpaired older adults with CVD, this study aimed to determine ante-mortem cognitive trajectories associated with elevated Aβ and/or tau at autopsy.</p><p><strong>Methods: </strong>Participants aged 65-95 classified as cognitively unimpaired at baseline from the National Alzheimer's Coordinating Center database, with ≥ 1 follow-up between 2005 and 2015, and available autopsy/APOE data were included in this cohort study (N = 863). All participants had at least one of six CVD markers at autopsy. Participants were classified into four groups (A - T-, A + T-, A - T+, A + T+) based on semiquantitative Consortium to Establish a Registry for Alzheimer's Disease neuritic plaque staging and Braak staging. Linear mixed models assessed rate of change in Preclinical Alzheimer's Cognitive Composite scores, episodic memory, and executive function.</p><p><strong>Results: </strong>A + T + adults demonstrated significantly faster cognitive decline on all outcomes in the ~ 10 years preceding death compared to A - T- adults (d = 0.34-0.46). Similarly, when compared to A + T - adults, A + T + adults showed significantly faster decline on all outcomes (d = 0.19-0.37). At the last visit prior to death, a greater proportion of A + T + adults (36%) received a dementia diagnosis compared to A - T+ (15%; OR = 6.00), A + T- (14%; OR = 8.00) and A - T- adults (12%; OR = 6.86), p <.001. When analyses were restricted to exclude dementia diagnoses, significantly faster decline on all outcomes (p's < 0.001, d = 0.29-0.37) was similarly observed in A + T + adults compared to A - T- adults.</p><p><strong>Conclusions: </strong>In older adults with concurrent CVD, A + T + at autopsy was associated with greater cognitive decline over 10 years preceding death compared to A - T- older adults. Faster cognitive decline in A + T + in the context of low final visit dementia diagnoses may suggest that post-mortem A + T + is associated with a steep trajectory of cognitive decline ante-mortem, but that dementia progression is not inevitable.</p>\",\"PeriodicalId\":7516,\"journal\":{\"name\":\"Alzheimer's Research & Therapy\",\"volume\":\"17 1\",\"pages\":\"165\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2025-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12273324/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Alzheimer's Research & Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13195-025-01776-w\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Alzheimer's Research & Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13195-025-01776-w","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:β -淀粉样蛋白(β)斑块和tau蛋白缠结是阿尔茨海默病(AD)的病理标志;然而,尸检研究显示,大多数老年人也存在脑血管疾病(CVD)标志物。目前尚不清楚在并发CVD的情况下,Aβ和tau如何与认知相关。在最初认知功能未受损的CVD老年人中,本研究旨在确定尸检时与Aβ和/或tau升高相关的死前认知轨迹。方法:从国家阿尔茨海默病协调中心数据库中,年龄在65-95岁的受试者在基线时被分类为认知未受损,在2005年至2015年期间进行了≥1次随访,并纳入了现有的尸检/APOE数据(N = 863)。所有参与者在尸检时至少有六种心血管疾病标志物中的一种。参与者被分为四组(A - T-, A + T-, A - T+, A + T+)基于半定量联盟建立阿尔茨海默病神经斑块分期和Braak分期登记。线性混合模型评估临床前阿尔茨海默氏症认知综合评分、情景记忆和执行功能的变化率。结果:与A - T组相比,A + T组成人在死亡前10年的所有结果中表现出明显更快的认知衰退(d = 0.34-0.46)。同样,与A + T -成人相比,A + T +成人在所有结果上的下降都明显更快(d = 0.19-0.37)。在死亡前的最后一次访问中,与a - T+(15%)相比,a + T+成人(36%)接受痴呆诊断的比例更高;Or = 6.00), a + t - (14%;OR = 8.00)和A - T-成人(12%;OR = 6.86), p结论:在并发CVD的老年人中,与A - T老年人相比,尸检时A + T +与死亡前10年更大的认知能力下降有关。在低临终痴呆诊断的背景下,A + T +的认知能力下降更快,这可能表明死后A + T +与死前认知能力下降的急剧轨迹有关,但痴呆的进展并非不可避免。
Ante-mortem cognitive trajectories associated with Aβ and tau biomarker profiles in older adults with cerebrovascular disease: a longitudinal cohort study.
Background: Beta-amyloid (Aβ) plaques and tau tangles are pathological hallmarks of Alzheimer's disease (AD); however, autopsy studies reveal that most older adults also present with cerebrovascular disease (CVD) markers. It remains unclear how Aβ and tau relate to cognition in the context of concurrent CVD. In initially cognitively unimpaired older adults with CVD, this study aimed to determine ante-mortem cognitive trajectories associated with elevated Aβ and/or tau at autopsy.
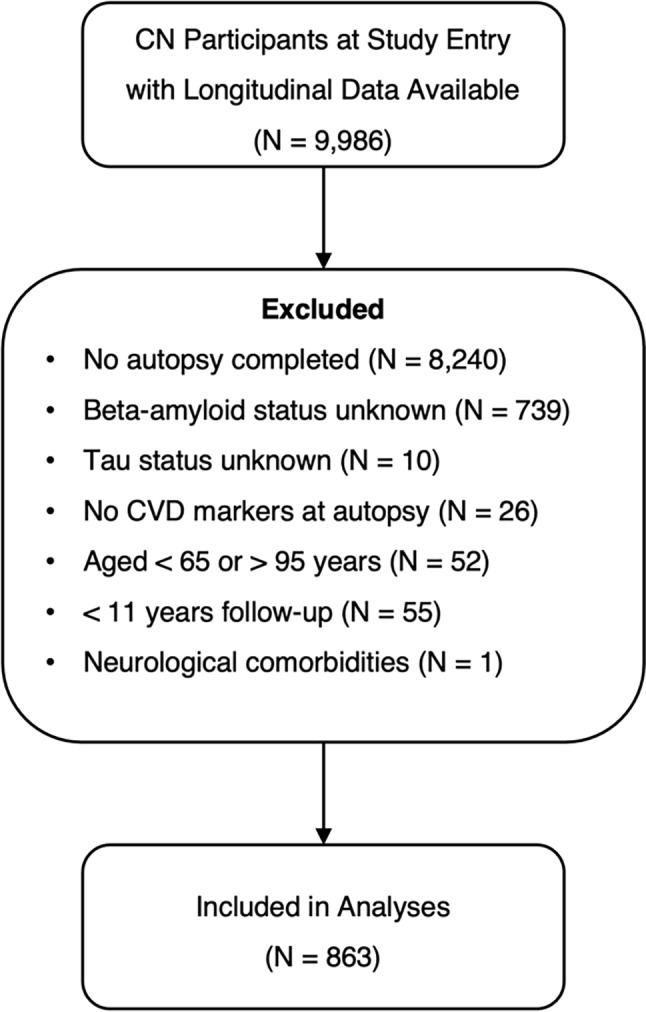
Methods: Participants aged 65-95 classified as cognitively unimpaired at baseline from the National Alzheimer's Coordinating Center database, with ≥ 1 follow-up between 2005 and 2015, and available autopsy/APOE data were included in this cohort study (N = 863). All participants had at least one of six CVD markers at autopsy. Participants were classified into four groups (A - T-, A + T-, A - T+, A + T+) based on semiquantitative Consortium to Establish a Registry for Alzheimer's Disease neuritic plaque staging and Braak staging. Linear mixed models assessed rate of change in Preclinical Alzheimer's Cognitive Composite scores, episodic memory, and executive function.
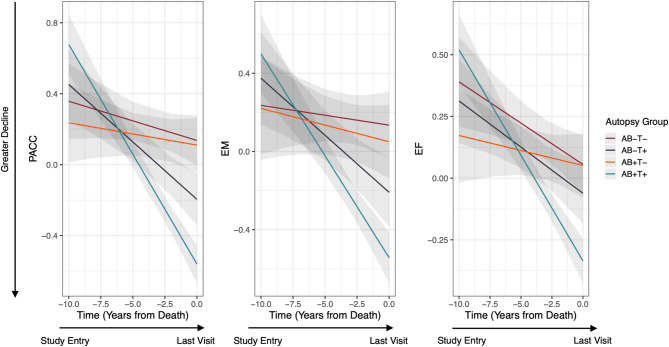
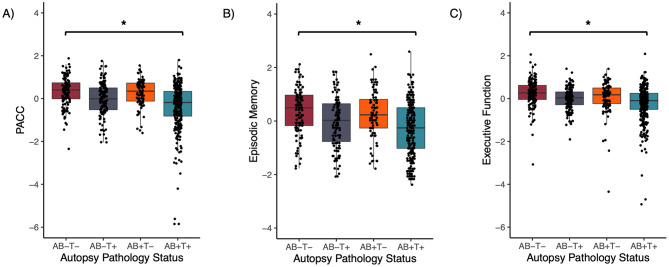
Results: A + T + adults demonstrated significantly faster cognitive decline on all outcomes in the ~ 10 years preceding death compared to A - T- adults (d = 0.34-0.46). Similarly, when compared to A + T - adults, A + T + adults showed significantly faster decline on all outcomes (d = 0.19-0.37). At the last visit prior to death, a greater proportion of A + T + adults (36%) received a dementia diagnosis compared to A - T+ (15%; OR = 6.00), A + T- (14%; OR = 8.00) and A - T- adults (12%; OR = 6.86), p <.001. When analyses were restricted to exclude dementia diagnoses, significantly faster decline on all outcomes (p's < 0.001, d = 0.29-0.37) was similarly observed in A + T + adults compared to A - T- adults.
Conclusions: In older adults with concurrent CVD, A + T + at autopsy was associated with greater cognitive decline over 10 years preceding death compared to A - T- older adults. Faster cognitive decline in A + T + in the context of low final visit dementia diagnoses may suggest that post-mortem A + T + is associated with a steep trajectory of cognitive decline ante-mortem, but that dementia progression is not inevitable.
期刊介绍:
Alzheimer's Research & Therapy is an international peer-reviewed journal that focuses on translational research into Alzheimer's disease and other neurodegenerative diseases. It publishes open-access basic research, clinical trials, drug discovery and development studies, and epidemiologic studies. The journal also includes reviews, viewpoints, commentaries, debates, and reports. All articles published in Alzheimer's Research & Therapy are included in several reputable databases such as CAS, Current contents, DOAJ, Embase, Journal Citation Reports/Science Edition, MEDLINE, PubMed, PubMed Central, Science Citation Index Expanded (Web of Science) and Scopus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


