{"title":"医疗保险受益人社会风险记录的测量偏倚。","authors":"Paula Chatterjee, Eliza Macneal, Eric T Roberts","doi":"10.1001/jamahealthforum.2025.1923","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Health care organizations are increasingly measuring social risk using Z codes. Types of social risk captured in Z codes include issues related to employment, housing, education, or other psychosocial circumstances. Prior work has found low use of Z codes overall, but measurement may be biased in other ways that have implications for risk adjustment and resource allocation.</p><p><strong>Objective: </strong>To characterize Z code measurement among hospitalized Medicare beneficiaries across levels of clinical complexity and historical health care utilization and examine implications of these patterns for mortality prediction.</p><p><strong>Design, setting, and participants: </strong>This retrospective cohort study included Medicare beneficiaries with an inpatient hospital admission in 2022. Data were analyzed from May 2024 to June 2025.</p><p><strong>Main outcomes and measurements: </strong>Presence of Z codes (codes Z55 to Z65) in any diagnosis field for a hospital admission, variation in Z code documentation across beneficiaries categorized by clinical risk (Elixhauser Comorbidity Index risk scores and predicted 30-day mortality risk) and historical utilization levels (number of hospitalizations in the prior year), and the association between Z code documentation and observed 30-day mortality, controlling for hospital fixed effects.</p><p><strong>Results: </strong>Among 7 069 611 hospitalized Medicare beneficiaries in 2022, 3 816 420 (54.0%) were female, and 6 093 932 (86.1%) were 65 years or older. A total of 148 592 (2.1%) had at least 1 Z code on the index hospital claim. Within-hospital Z code prevalence was higher for beneficiaries with lower Elixhauser Comorbidity Index clinical risk scores (2.8% vs 1.5%) and higher among patients with at least 2 hospitalizations in the prior year (2.6%) than patients with zero (1.8%) or 1 (2.1%) prior hospitalizations. Despite known population-level associations between social risk and increased mortality, Z code prevalence was highest among beneficiaries with the lowest predicted 30-day mortality risk (4.4%) and lowest among beneficiaries with the highest mortality risk (1.6%). Correspondingly, in within-hospital analyses that did not adjust for patient-level covariates such as demographic characteristics and clinical risk, the presence of a Z code was associated with a lower probability of observed 30-day mortality (5.1% vs 4.2%; difference, -0.9 percentage points; 95% CI, -1.0 to -0.8).</p><p><strong>Conclusions and relevance: </strong>This cohort study found that Z code use patterns likely underrepresent social risk among clinically complex patients, resulting in a spurious negative association between documented social risk and mortality. Alternative socioeconomic indicators, including data collected for population and public health surveillance, may offer more reliable measures of social risk than Z codes.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 7","pages":"e251923"},"PeriodicalIF":11.3000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12274977/pdf/","citationCount":"0","resultStr":"{\"title\":\"Measurement Bias in Documentation of Social Risk Among Medicare Beneficiaries.\",\"authors\":\"Paula Chatterjee, Eliza Macneal, Eric T Roberts\",\"doi\":\"10.1001/jamahealthforum.2025.1923\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Health care organizations are increasingly measuring social risk using Z codes. Types of social risk captured in Z codes include issues related to employment, housing, education, or other psychosocial circumstances. Prior work has found low use of Z codes overall, but measurement may be biased in other ways that have implications for risk adjustment and resource allocation.</p><p><strong>Objective: </strong>To characterize Z code measurement among hospitalized Medicare beneficiaries across levels of clinical complexity and historical health care utilization and examine implications of these patterns for mortality prediction.</p><p><strong>Design, setting, and participants: </strong>This retrospective cohort study included Medicare beneficiaries with an inpatient hospital admission in 2022. Data were analyzed from May 2024 to June 2025.</p><p><strong>Main outcomes and measurements: </strong>Presence of Z codes (codes Z55 to Z65) in any diagnosis field for a hospital admission, variation in Z code documentation across beneficiaries categorized by clinical risk (Elixhauser Comorbidity Index risk scores and predicted 30-day mortality risk) and historical utilization levels (number of hospitalizations in the prior year), and the association between Z code documentation and observed 30-day mortality, controlling for hospital fixed effects.</p><p><strong>Results: </strong>Among 7 069 611 hospitalized Medicare beneficiaries in 2022, 3 816 420 (54.0%) were female, and 6 093 932 (86.1%) were 65 years or older. A total of 148 592 (2.1%) had at least 1 Z code on the index hospital claim. Within-hospital Z code prevalence was higher for beneficiaries with lower Elixhauser Comorbidity Index clinical risk scores (2.8% vs 1.5%) and higher among patients with at least 2 hospitalizations in the prior year (2.6%) than patients with zero (1.8%) or 1 (2.1%) prior hospitalizations. Despite known population-level associations between social risk and increased mortality, Z code prevalence was highest among beneficiaries with the lowest predicted 30-day mortality risk (4.4%) and lowest among beneficiaries with the highest mortality risk (1.6%). Correspondingly, in within-hospital analyses that did not adjust for patient-level covariates such as demographic characteristics and clinical risk, the presence of a Z code was associated with a lower probability of observed 30-day mortality (5.1% vs 4.2%; difference, -0.9 percentage points; 95% CI, -1.0 to -0.8).</p><p><strong>Conclusions and relevance: </strong>This cohort study found that Z code use patterns likely underrepresent social risk among clinically complex patients, resulting in a spurious negative association between documented social risk and mortality. Alternative socioeconomic indicators, including data collected for population and public health surveillance, may offer more reliable measures of social risk than Z codes.</p>\",\"PeriodicalId\":53180,\"journal\":{\"name\":\"JAMA Health Forum\",\"volume\":\"6 7\",\"pages\":\"e251923\"},\"PeriodicalIF\":11.3000,\"publicationDate\":\"2025-07-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12274977/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Health Forum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1001/jamahealthforum.2025.1923\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2025.1923","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
摘要
重要性:卫生保健组织越来越多地使用Z代码来衡量社会风险。在Z代码中捕获的社会风险类型包括与就业、住房、教育或其他社会心理环境有关的问题。先前的工作发现总体上Z码的使用率很低,但测量可能在其他方面有偏差,这对风险调整和资源分配有影响。目的:研究住院医疗保险受益人临床复杂性和历史医疗保健利用水平的Z码测量特征,并研究这些模式对死亡率预测的影响。设计、环境和参与者:这项回顾性队列研究包括2022年住院的医疗保险受益人。数据分析时间为2024年5月至2025年6月。主要结果和测量:在住院的任何诊断领域存在Z代码(代码Z55至Z65),按临床风险(Elixhauser共病指数风险评分和预测的30天死亡风险)和历史利用水平(前一年住院次数)分类的受益人之间Z代码文件的差异,以及Z代码文件与观察到的30天死亡率之间的关联,控制了医院固定效应。结果:2022年住院医保受益人7 069 611人中,女性3 816 420人(54.0%),65岁及以上6 093 932人(86.1%)。148名 592名(2.1%)患者在指标医院理赔上至少有1个Z码。院内Z码患病率在Elixhauser合并症指数临床风险评分较低的受益人中较高(2.8% vs 1.5%),在前一年至少住院2次的患者中(2.6%)高于无住院史(1.8%)或1次住院史(2.1%)的患者。尽管已知社会风险与死亡率增加之间存在人口层面的关联,但Z代码患病率在预测30天死亡率风险最低的受益人中最高(4.4%),在死亡率风险最高的受益人中最低(1.6%)。相应地,在没有调整患者水平协变量(如人口统计学特征和临床风险)的院内分析中,Z代码的存在与观察到的30天死亡率较低的概率相关(5.1% vs 4.2%;差异为-0.9个百分点;95% CI, -1.0至-0.8)。结论和相关性:该队列研究发现,Z码使用模式可能未充分代表临床复杂患者的社会风险,导致记录的社会风险与死亡率之间存在虚假的负相关。其他社会经济指标,包括为人口和公共卫生监测收集的数据,可能比Z码提供更可靠的社会风险衡量指标。
Measurement Bias in Documentation of Social Risk Among Medicare Beneficiaries.
Importance: Health care organizations are increasingly measuring social risk using Z codes. Types of social risk captured in Z codes include issues related to employment, housing, education, or other psychosocial circumstances. Prior work has found low use of Z codes overall, but measurement may be biased in other ways that have implications for risk adjustment and resource allocation.
Objective: To characterize Z code measurement among hospitalized Medicare beneficiaries across levels of clinical complexity and historical health care utilization and examine implications of these patterns for mortality prediction.
Design, setting, and participants: This retrospective cohort study included Medicare beneficiaries with an inpatient hospital admission in 2022. Data were analyzed from May 2024 to June 2025.
Main outcomes and measurements: Presence of Z codes (codes Z55 to Z65) in any diagnosis field for a hospital admission, variation in Z code documentation across beneficiaries categorized by clinical risk (Elixhauser Comorbidity Index risk scores and predicted 30-day mortality risk) and historical utilization levels (number of hospitalizations in the prior year), and the association between Z code documentation and observed 30-day mortality, controlling for hospital fixed effects.
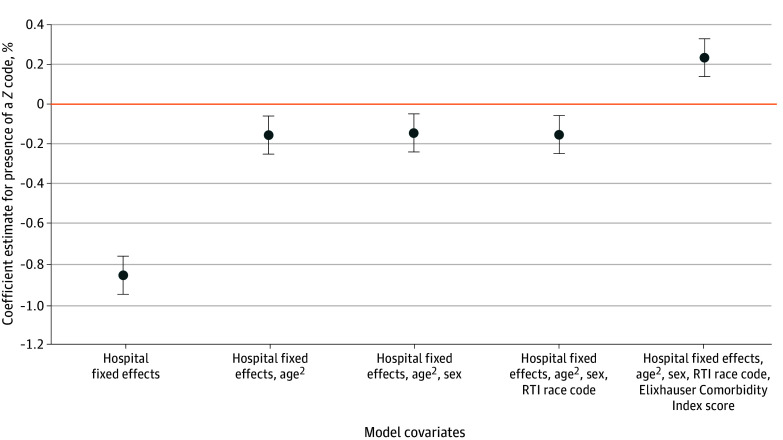
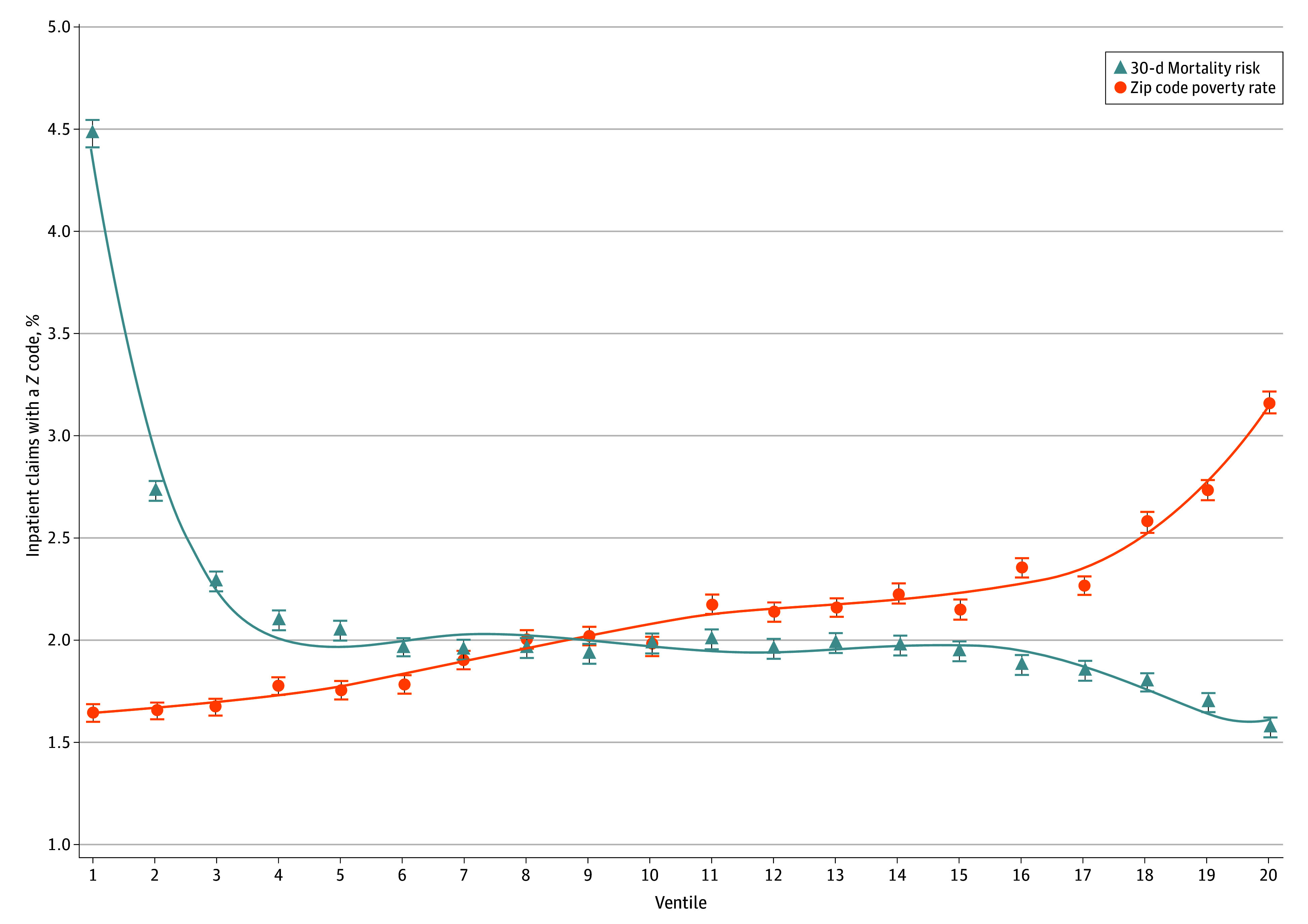
Results: Among 7 069 611 hospitalized Medicare beneficiaries in 2022, 3 816 420 (54.0%) were female, and 6 093 932 (86.1%) were 65 years or older. A total of 148 592 (2.1%) had at least 1 Z code on the index hospital claim. Within-hospital Z code prevalence was higher for beneficiaries with lower Elixhauser Comorbidity Index clinical risk scores (2.8% vs 1.5%) and higher among patients with at least 2 hospitalizations in the prior year (2.6%) than patients with zero (1.8%) or 1 (2.1%) prior hospitalizations. Despite known population-level associations between social risk and increased mortality, Z code prevalence was highest among beneficiaries with the lowest predicted 30-day mortality risk (4.4%) and lowest among beneficiaries with the highest mortality risk (1.6%). Correspondingly, in within-hospital analyses that did not adjust for patient-level covariates such as demographic characteristics and clinical risk, the presence of a Z code was associated with a lower probability of observed 30-day mortality (5.1% vs 4.2%; difference, -0.9 percentage points; 95% CI, -1.0 to -0.8).
Conclusions and relevance: This cohort study found that Z code use patterns likely underrepresent social risk among clinically complex patients, resulting in a spurious negative association between documented social risk and mortality. Alternative socioeconomic indicators, including data collected for population and public health surveillance, may offer more reliable measures of social risk than Z codes.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


