{"title":"帕金森病药物治疗的现状和未来进展。","authors":"Thomas Müller","doi":"10.1007/s40120-025-00800-3","DOIUrl":null,"url":null,"abstract":"<p><p>Symptomatic drug treatment of Parkinson's disease combines various pharmacological principles for a patient-tailored drug combination. Development of more continuous delivery modes of dopamine-substituting drugs with formulations with better pharmacokinetic properties has enabled less frequent dosing and thereby provided further benefit for patients. Peripheral weakening of dopa decarboxylase activity with nutrients, such as short fatty acids, may enhance levodopa efficacy. A future concept may be mandatory combined central inhibition of catechol-O-methyltransferase, monoamine oxidase B and tyrosinase in levodopa-treated patients, if tolerated. This approach may hypothetically protect against toxins resulting from catecholamine metabolism. Beneficial modification of disease progression and cure is an unmet need. High expectations were mainly generated by promising positive experimental research outcomes. The employed models of Parkinson's disease provide uniform trial conditions. Drug safety and the side effect profile have minor importance. Subsequently performed translational clinical trials failed. Examples are studies with iron chelators, glucagon-like peptide 1 receptor agonists and free radical scavengers, particularly when levodopa-naïve patients were included. Multifactorial heterogeneity of disease mechanisms, variability of symptoms and their progression are the main causes for these negative results. Additionally an impact of symptomatic dopamine-substituting treatments on the course of Parkinson's disease was demonstrated in clinical studies with monoamine oxidase B inhibitors and dopamine agonists with levodopa therapy as comparator. Neuron transplantation, application of stem cells and their secreted exosomes, or secretomes, are still mainly considered by experimental researchers. Translation into clinical practice is complex or has failed. Stimulation of an existing endogenous repair system in the peripheral and central nervous system is an alternative. Repulsive guidance molecule A (RGMa) inhibits physiologic regeneration in peripheral and central neurons. Blocking of the physiologic effects of this protein initiates endogenous repair in models of acute and chronic neuronal dying as a more general therapeutic concept for chronic neurodegenerative and inflammatory disease.</p>","PeriodicalId":19216,"journal":{"name":"Neurology and Therapy","volume":" ","pages":"1769-1781"},"PeriodicalIF":4.8000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450148/pdf/","citationCount":"0","resultStr":"{\"title\":\"Update on the Present and Future Pharmacologic Treatment of Parkinson's Disease.\",\"authors\":\"Thomas Müller\",\"doi\":\"10.1007/s40120-025-00800-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Symptomatic drug treatment of Parkinson's disease combines various pharmacological principles for a patient-tailored drug combination. Development of more continuous delivery modes of dopamine-substituting drugs with formulations with better pharmacokinetic properties has enabled less frequent dosing and thereby provided further benefit for patients. Peripheral weakening of dopa decarboxylase activity with nutrients, such as short fatty acids, may enhance levodopa efficacy. A future concept may be mandatory combined central inhibition of catechol-O-methyltransferase, monoamine oxidase B and tyrosinase in levodopa-treated patients, if tolerated. This approach may hypothetically protect against toxins resulting from catecholamine metabolism. Beneficial modification of disease progression and cure is an unmet need. High expectations were mainly generated by promising positive experimental research outcomes. The employed models of Parkinson's disease provide uniform trial conditions. Drug safety and the side effect profile have minor importance. Subsequently performed translational clinical trials failed. Examples are studies with iron chelators, glucagon-like peptide 1 receptor agonists and free radical scavengers, particularly when levodopa-naïve patients were included. Multifactorial heterogeneity of disease mechanisms, variability of symptoms and their progression are the main causes for these negative results. Additionally an impact of symptomatic dopamine-substituting treatments on the course of Parkinson's disease was demonstrated in clinical studies with monoamine oxidase B inhibitors and dopamine agonists with levodopa therapy as comparator. Neuron transplantation, application of stem cells and their secreted exosomes, or secretomes, are still mainly considered by experimental researchers. Translation into clinical practice is complex or has failed. Stimulation of an existing endogenous repair system in the peripheral and central nervous system is an alternative. Repulsive guidance molecule A (RGMa) inhibits physiologic regeneration in peripheral and central neurons. Blocking of the physiologic effects of this protein initiates endogenous repair in models of acute and chronic neuronal dying as a more general therapeutic concept for chronic neurodegenerative and inflammatory disease.</p>\",\"PeriodicalId\":19216,\"journal\":{\"name\":\"Neurology and Therapy\",\"volume\":\" \",\"pages\":\"1769-1781\"},\"PeriodicalIF\":4.8000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450148/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology and Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40120-025-00800-3\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40120-025-00800-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/18 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
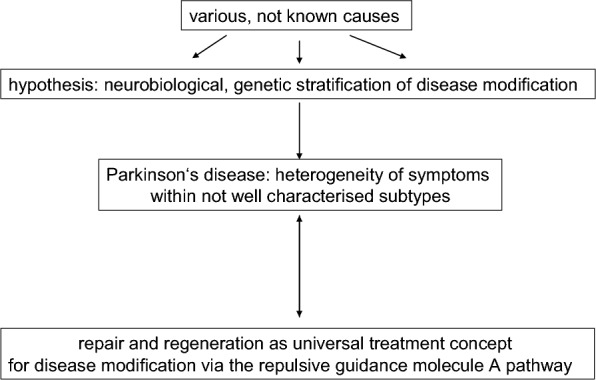
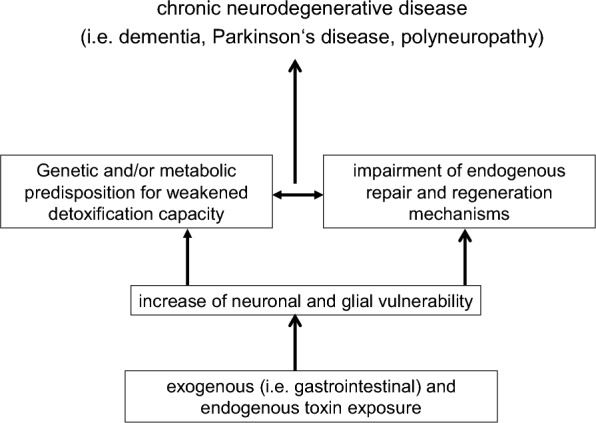
帕金森病的对症药物治疗结合了各种药理学原理,为患者量身定制药物组合。开发具有更好药代动力学特性的配方的多巴胺替代药物的更连续递送模式,使给药频率降低,从而为患者提供进一步的益处。外周多巴脱羧酶活性随着营养物质(如短脂肪酸)的减弱而减弱,可能会增强左旋多巴的疗效。一个未来的概念可能是强制联合中枢抑制儿茶酚- o -甲基转移酶,单胺氧化酶B和酪氨酸酶在左旋多巴治疗的患者,如果耐受。这种方法可以防止由儿茶酚胺代谢产生的毒素。对疾病进展和治疗的有益改变是一个未满足的需求。高期望值主要来自于有希望的积极的实验研究成果。所采用的帕金森病模型提供了统一的试验条件。药物安全性和副作用不太重要。随后进行的转化临床试验均以失败告终。例如铁螯合剂、胰高血糖素样肽1受体激动剂和自由基清除剂的研究,特别是当levodopa-naïve患者被纳入研究时。疾病机制的多因素异质性、症状及其进展的可变性是这些阴性结果的主要原因。此外,在单胺氧化酶B抑制剂和多巴胺激动剂与左旋多巴治疗作为比较的临床研究中,证明了症状性多巴胺替代治疗对帕金森病病程的影响。神经元移植、干细胞及其分泌的外泌体(secretomes)的应用仍是实验研究者主要考虑的问题。将其转化为临床实践是复杂的或失败的。刺激周围和中枢神经系统的内源性修复系统是另一种选择。排斥引导分子A (RGMa)抑制外周和中枢神经元的生理性再生。阻断该蛋白的生理作用在急性和慢性神经元死亡模型中启动内源性修复,作为慢性神经退行性和炎症性疾病的更普遍的治疗概念。
Update on the Present and Future Pharmacologic Treatment of Parkinson's Disease.
Symptomatic drug treatment of Parkinson's disease combines various pharmacological principles for a patient-tailored drug combination. Development of more continuous delivery modes of dopamine-substituting drugs with formulations with better pharmacokinetic properties has enabled less frequent dosing and thereby provided further benefit for patients. Peripheral weakening of dopa decarboxylase activity with nutrients, such as short fatty acids, may enhance levodopa efficacy. A future concept may be mandatory combined central inhibition of catechol-O-methyltransferase, monoamine oxidase B and tyrosinase in levodopa-treated patients, if tolerated. This approach may hypothetically protect against toxins resulting from catecholamine metabolism. Beneficial modification of disease progression and cure is an unmet need. High expectations were mainly generated by promising positive experimental research outcomes. The employed models of Parkinson's disease provide uniform trial conditions. Drug safety and the side effect profile have minor importance. Subsequently performed translational clinical trials failed. Examples are studies with iron chelators, glucagon-like peptide 1 receptor agonists and free radical scavengers, particularly when levodopa-naïve patients were included. Multifactorial heterogeneity of disease mechanisms, variability of symptoms and their progression are the main causes for these negative results. Additionally an impact of symptomatic dopamine-substituting treatments on the course of Parkinson's disease was demonstrated in clinical studies with monoamine oxidase B inhibitors and dopamine agonists with levodopa therapy as comparator. Neuron transplantation, application of stem cells and their secreted exosomes, or secretomes, are still mainly considered by experimental researchers. Translation into clinical practice is complex or has failed. Stimulation of an existing endogenous repair system in the peripheral and central nervous system is an alternative. Repulsive guidance molecule A (RGMa) inhibits physiologic regeneration in peripheral and central neurons. Blocking of the physiologic effects of this protein initiates endogenous repair in models of acute and chronic neuronal dying as a more general therapeutic concept for chronic neurodegenerative and inflammatory disease.
期刊介绍:
Aims and Scope
Neurology and Therapy aims to provide reliable and inclusive, rapid publication for all therapy related research for neurological indications, supporting the timely dissemination of research with a global reach, to help advance scientific discovery and support clinical practice.
Neurology and Therapy is an international, open access, peer reviewed, rapid publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world and health outcomes research around the discovery, development, and use of neurological and psychiatric therapies, (also covering surgery and devices). Studies relating to diagnosis, pharmacoeconomics, public health, quality of life, and patient care, management, and education are also welcomed.
The journal is of interest to a broad audience of healthcare professionals and publishes original research, reviews, case reports, trial designs, communications and letters. The journal is read by a global audience and receives submissions from all over the world. Neurology and Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of all scientifically and ethically sound research.
Rapid Publication
The journal’s rapid publication timelines aim for a peer review decision within 2 weeks of submission. If an article is accepted, it will be published online 3-4 weeks from acceptance. These rapid timelines are achieved through the combination of a dedicated in-house editorial team, who closely manage article workflow, and an extensive Editorial and Advisory Board who assist with rapid peer review. This allows the journal to support the rapid dissemination of research, whilst still providing robust peer review. Combined with the journal’s open access model, this allows for the rapid and efficient communication of the latest research and reviews to support scientific discovery and clinical practice.
Open Access
All articles published by Neurology and Therapy are open access.
Personal Service
The journal’s dedicated in-house editorial team offer a personal “concierge service” meaning that authors will always have a personal point of contact able to update them on the status of their manuscript. The editorial team check all manuscripts to ensure that articles conform to the most recent COPE and ICMJE publishing guidelines. This supports the publication of ethically sound and transparent research. We also encourage pre-submission enquiries and are always happy to provide a confidential assessment of manuscripts.
Digital Features and Plain Language Summaries
Neurology and Therapy offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by key summary points, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article. The journal also provides the option to include various types of digital features including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations. All additional features are peer reviewed to the same high standard as the article itself. If you consider that your paper would benefit from the inclusion of a digital feature, please let us know. Our editorial team are able to create high-quality slide decks and infographics in-house, and video abstracts through our partner Research Square, and would be happy to assist in any way we can. For further information about digital features, please contact the journal editor (see ‘Contact the Journal’ for email address), and see the ‘Guidelines for digital features and plain language summaries’ document under ‘Submission guidelines’.
For examples of digital features please visit our showcase page https://springerhealthcare.com/expertise/publishing-digital-features/
Publication Fees
Upon acceptance of an article, authors will be required to pay the mandatory Rapid Service Fee of €5250/$6000/£4300. The journal will consider fee discounts and waivers for developing countries and this is decided on a case-by-case basis.
Peer Review Process
Upon submission, manuscripts are assessed by the editorial team to ensure they fit within the aims and scope of the journal and are also checked for plagiarism. All suitable submissions are then subject to a comprehensive single-blind peer review. Reviewers are selected based on their relevant expertise and publication history in the subject area. The journal has an extensive pool of editorial and advisory board members who have been selected to assist with peer review based on the afore-mentioned criteria.
At least two extensive reviews are required to make the editorial decision, with the exception of some article types such as Commentaries, Editorials and Letters which are generally reviewed by one member of the Editorial Board. Where reviews conflict, an Editorial Board Member will be contacted for further advice and a presiding decision. Manuscripts are then either accepted, rejected or authors are required to make major or minor revisions (both reviewer comments and editorial comments may need to be addressed. Once a revised manuscript is re-submitted, it is assessed along with the responses to reviewer comments and if it has been adequately revised, it will be accepted for publication. Accepted manuscripts are then copyedited and typeset by the production team before online publication. Appeals against decisions following peer review are considered on a case-by-case basis and should be sent to the journal editor, and authors are welcome to make rebuttals against individual reviewer comments, if appropriate.
Preprints
We encourage posting of preprints of primary research manuscripts on preprint servers, authors'' or institutional websites, and open communications between researchers whether on community preprint servers or preprint commenting platforms. Posting of preprints is not considered prior publication and will not jeopardize consideration in our journals.
Please see here for further information on preprint sharing: https://www.springer.com/gp/authors-editors/journal-author/journal-author-helpdesk/submission/1302#c16721550
Copyright
Neurology and Therapy is published under the Creative Commons Attribution-Noncommercial License, which allows users to read, copy, distribute, and make derivative works for non-commercial purposes from the material, as long as the author of the original work is cited. The author assigns the exclusive right to any commercial use of the article to Springer. For more information about the Creative Commons Attribution-Noncommercial License, click here: http://creativecommons.org/licenses/by-nc/4.0.
Contact
For more information about the journal, including pre-submission enquiries, please contact managing editor Lydia Alborn at lydia.alborn@springer.com.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


