Márton Boga, Zoltán Salló, Gábor Orbán, Ferenc Komlósi, Anna Padisák, Patrik Tóth, Péter Perge, Vivien Klaudia Nagy, Edit Tanai, István Osztheimer, Béla Merkely, László Gellér, Nándor Szegedi
{"title":"对持续性房颤导管消融前电复律反应的影响:倾向评分匹配分析。","authors":"Márton Boga, Zoltán Salló, Gábor Orbán, Ferenc Komlósi, Anna Padisák, Patrik Tóth, Péter Perge, Vivien Klaudia Nagy, Edit Tanai, István Osztheimer, Béla Merkely, László Gellér, Nándor Szegedi","doi":"10.1093/ehjopen/oeaf084","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>We hypothesize that sinus rhythm (SR) maintenance in persistent atrial fibrillation (AF) patients taking anti-arrhythmic drugs (AADs) after pre-procedural electrical cardioversion (ECV) could predict outcomes after catheter ablation procedures.</p><p><strong>Methods and results: </strong>219 persistent AF patients on AADs underwent ECV 1-6 months before ablation. Patients were categorized into two groups according to their response to ECV: patients in whom SR was restored and maintained until the ablation procedure (ECV-SR group), and patients with AF recurrence before the procedure (ECV-AF group). Then, 1:1 propensity score matching was used to create study groups (94-94 patients). The efficacy outcomes of the present study were freedom from atrial tachyarrhythmia on/off AADs following a single ablation procedure and recurrence of persistent AF. The median follow-up duration was 42 (20-73) months. Freedom from atrial tachyarrhythmia at 36 months was lower in the ECV-AF group compared to ECV-SR patients (31.4% vs. 51.2%, respectively; crude HR = 2.58, 95% CI = 1.58-3.70, <i>P</i> < 0.001). The most frequent pattern of atrial arrhythmia recurrence was persistent AF in the ECV-AF group and paroxysmal AF in the ECV-SR group. Freedom from persistent AF at 36 months was 54% and 84.3%, respectively (crude HR = 3.72, 95% CI = 1.94-7.14, <i>P</i> < 0.001). Differences in the risk of the efficacy outcomes were similar after multi-variable adjustment and in all analysed subgroups, including pulmonary vein isolation (PVI)-only procedures.</p><p><strong>Conclusion: </strong>Our findings indicate that the positive response to pre-procedural ECV may be a valuable marker for identifying persistent AF patients in whom a PVI-only strategy is sufficient.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 4","pages":"oeaf084"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12264425/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of response to electrical cardioversion before catheter ablation for persistent atrial fibrillation: a propensity score-matched analysis.\",\"authors\":\"Márton Boga, Zoltán Salló, Gábor Orbán, Ferenc Komlósi, Anna Padisák, Patrik Tóth, Péter Perge, Vivien Klaudia Nagy, Edit Tanai, István Osztheimer, Béla Merkely, László Gellér, Nándor Szegedi\",\"doi\":\"10.1093/ehjopen/oeaf084\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>We hypothesize that sinus rhythm (SR) maintenance in persistent atrial fibrillation (AF) patients taking anti-arrhythmic drugs (AADs) after pre-procedural electrical cardioversion (ECV) could predict outcomes after catheter ablation procedures.</p><p><strong>Methods and results: </strong>219 persistent AF patients on AADs underwent ECV 1-6 months before ablation. Patients were categorized into two groups according to their response to ECV: patients in whom SR was restored and maintained until the ablation procedure (ECV-SR group), and patients with AF recurrence before the procedure (ECV-AF group). Then, 1:1 propensity score matching was used to create study groups (94-94 patients). The efficacy outcomes of the present study were freedom from atrial tachyarrhythmia on/off AADs following a single ablation procedure and recurrence of persistent AF. The median follow-up duration was 42 (20-73) months. Freedom from atrial tachyarrhythmia at 36 months was lower in the ECV-AF group compared to ECV-SR patients (31.4% vs. 51.2%, respectively; crude HR = 2.58, 95% CI = 1.58-3.70, <i>P</i> < 0.001). The most frequent pattern of atrial arrhythmia recurrence was persistent AF in the ECV-AF group and paroxysmal AF in the ECV-SR group. Freedom from persistent AF at 36 months was 54% and 84.3%, respectively (crude HR = 3.72, 95% CI = 1.94-7.14, <i>P</i> < 0.001). Differences in the risk of the efficacy outcomes were similar after multi-variable adjustment and in all analysed subgroups, including pulmonary vein isolation (PVI)-only procedures.</p><p><strong>Conclusion: </strong>Our findings indicate that the positive response to pre-procedural ECV may be a valuable marker for identifying persistent AF patients in whom a PVI-only strategy is sufficient.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 4\",\"pages\":\"oeaf084\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12264425/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf084\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf084","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:我们假设持续性心房颤动(AF)患者在术前电转复(ECV)后服用抗心律失常药物(AADs)维持窦性心律(SR)可以预测导管消融手术后的预后。方法与结果:219例AADs持续性房颤患者在消融前1 ~ 6个月行ECV治疗。根据患者对ECV的反应将患者分为两组:恢复并维持SR至消融手术的患者(ECV-SR组)和手术前AF复发的患者(ECV-AF组)。然后,采用1:1倾向评分匹配法创建研究组(94-94例)。本研究的疗效结果是在单次消融手术后无房性心动过速和持续性房颤复发。中位随访时间为42(20-73)个月。与ECV-SR患者相比,ECV-AF组在36个月时房性心动过速的自由度较低(分别为31.4%和51.2%;粗HR = 2.58, 95% CI = 1.58 ~ 3.70, P < 0.001)。房颤复发最常见的类型是ECV-AF组的持续性房颤和ECV-SR组的阵发性房颤。36个月时持续性房颤的发生率分别为54%和84.3%(粗HR = 3.72, 95% CI = 1.94-7.14, P < 0.001)。在多变量调整后,在所有分析的亚组中,包括仅肺静脉隔离(PVI)手术,疗效结果的风险差异相似。结论:我们的研究结果表明,术前ECV的阳性反应可能是识别持续性房颤患者的一个有价值的标志,在这些患者中,只有pvi策略是足够的。
Impact of response to electrical cardioversion before catheter ablation for persistent atrial fibrillation: a propensity score-matched analysis.
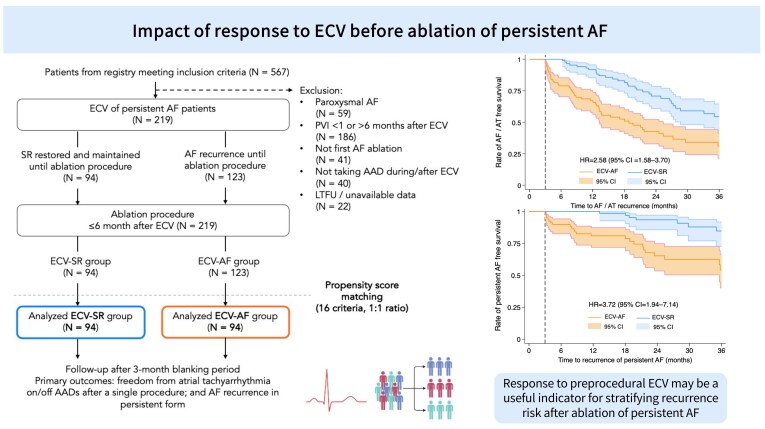
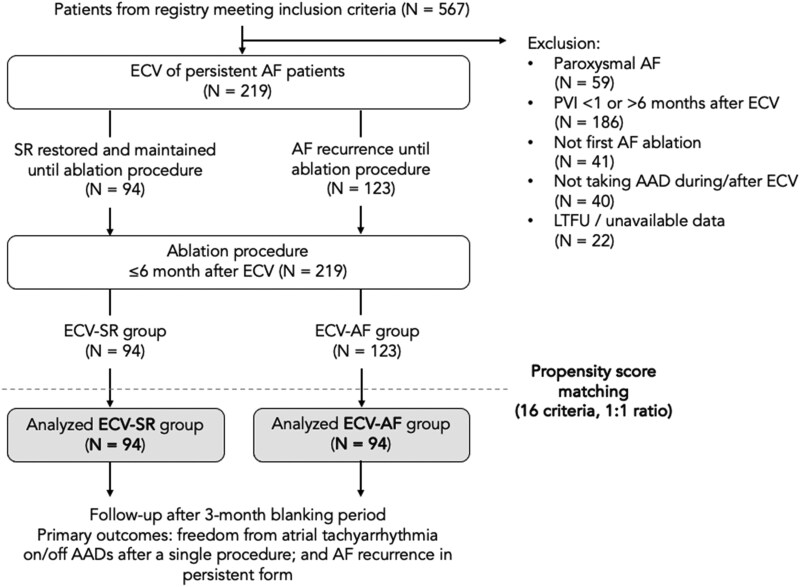
Aims: We hypothesize that sinus rhythm (SR) maintenance in persistent atrial fibrillation (AF) patients taking anti-arrhythmic drugs (AADs) after pre-procedural electrical cardioversion (ECV) could predict outcomes after catheter ablation procedures.
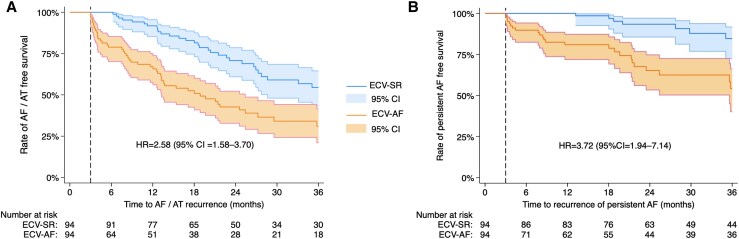
Methods and results: 219 persistent AF patients on AADs underwent ECV 1-6 months before ablation. Patients were categorized into two groups according to their response to ECV: patients in whom SR was restored and maintained until the ablation procedure (ECV-SR group), and patients with AF recurrence before the procedure (ECV-AF group). Then, 1:1 propensity score matching was used to create study groups (94-94 patients). The efficacy outcomes of the present study were freedom from atrial tachyarrhythmia on/off AADs following a single ablation procedure and recurrence of persistent AF. The median follow-up duration was 42 (20-73) months. Freedom from atrial tachyarrhythmia at 36 months was lower in the ECV-AF group compared to ECV-SR patients (31.4% vs. 51.2%, respectively; crude HR = 2.58, 95% CI = 1.58-3.70, P < 0.001). The most frequent pattern of atrial arrhythmia recurrence was persistent AF in the ECV-AF group and paroxysmal AF in the ECV-SR group. Freedom from persistent AF at 36 months was 54% and 84.3%, respectively (crude HR = 3.72, 95% CI = 1.94-7.14, P < 0.001). Differences in the risk of the efficacy outcomes were similar after multi-variable adjustment and in all analysed subgroups, including pulmonary vein isolation (PVI)-only procedures.
Conclusion: Our findings indicate that the positive response to pre-procedural ECV may be a valuable marker for identifying persistent AF patients in whom a PVI-only strategy is sufficient.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


