Jin Li, Qizhu Lin, Huangpeng Lin, Zexian Ma, Xuefeng Huang, Huimin Chen, Katsunori Sakamoto, Yongjie Su
{"title":"术前HELPP评分可以作为可切除胰腺癌患者的预后评估工具,也可能适用于中国患者。","authors":"Jin Li, Qizhu Lin, Huangpeng Lin, Zexian Ma, Xuefeng Huang, Huimin Chen, Katsunori Sakamoto, Yongjie Su","doi":"10.21037/gs-2025-132","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The incidence of pancreatic ductal adenocarcinoma (PDAC) is increasing annually, and the prognosis remains poor. There is currently no consensus on using neoadjuvant therapy for resectable pancreatic cancer. Further, existing preoperative prognostic scoring tools have notable limitations, making it challenging to identify patients who may benefit from neoadjuvant therapy. There is an urgent need for a widely recognized and effective tool to assess postoperative prognosis and guide treatment decisions. This study assessed and compared several widely used indicators, including the Heidelberg prognostic pancreatic cancer (HELPP) score, the Glasgow prognostic score (GPS), the systemic immune-inflammation index (SII), and the neutrophil-lymphocyte ratio (NLR).</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 61 pancreatic cancer patients who underwent radical resection at Zhongshan Hospital of Xiamen University from February 2015 to February 2022. The SII was calculated as (platelets × neutrophils/lymphocytes), and the NLR as (neutrophils/lymphocytes). The preoperative HELPP score was derived from American Society of Anesthesiologists (ASA) classification, carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), C-reactive protein (CRP), albumin, and platelets. The GPS was based on albumin and CRP levels. Optimal cut-off values for the quantitative data were established using Youden's index. Kaplan-Meier method and log-rank tests were used to categorize and group the HELPP scores. Univariate and multivariate survival analyses were conducted to explore the relationship between the HELPP score, GPS, SII, NLR, and postoperative survival of the pancreatic cancer patients. Chi-squared tests were used to compare the clinicopathological data across the prognostic score subgroups. The area under the receiver operating characteristic (ROC) curve (AUC) for each score was evaluated to assess predictive accuracy of 1- and 2-year survival.</p><p><strong>Results: </strong>The optimal cut-off values for the SII and NLR were 675.51 and 2.53, respectively. There were no significant differences in the survival times of the patients with HELPP scores of 1, 2, or 3 points (P>0.05); nor between those with scores of 4 and 5 points (P=0.058). The patients with preoperative HELPP scores of ≤3 points were allocated to the low HELPP score group, while those with scores >3 points were allocated to the high HELPP score group. A HELPP score >3 points, CEA ≥1.48 µg/L, and a tumor diameter >4 cm were found to be independent risk factors affecting postoperative prognosis (P<0.05). The SII, GPS, and NLR were not found to be significantly associated with prognosis. There were no statistically significant differences in the clinicopathological characteristics between the two HELPP score groups (P>0.05). The AUCs for overall survival (OS) for the HELPP score were 0.874 at 1 year and 0.696 at 2 years.</p><p><strong>Conclusions: </strong>The preoperative HELPP score is a promising tool for evaluating prognosis in patients with resectable pancreatic cancer, helpful in developing more appropriate preoperative treatment.</p>","PeriodicalId":12760,"journal":{"name":"Gland surgery","volume":"14 6","pages":"1112-1127"},"PeriodicalIF":1.6000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12261355/pdf/","citationCount":"0","resultStr":"{\"title\":\"The preoperative HELPP score can be used as a prognostic assessment tool for resectable pancreatic cancer patients, and may be applicable to patients in China as well.\",\"authors\":\"Jin Li, Qizhu Lin, Huangpeng Lin, Zexian Ma, Xuefeng Huang, Huimin Chen, Katsunori Sakamoto, Yongjie Su\",\"doi\":\"10.21037/gs-2025-132\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The incidence of pancreatic ductal adenocarcinoma (PDAC) is increasing annually, and the prognosis remains poor. There is currently no consensus on using neoadjuvant therapy for resectable pancreatic cancer. Further, existing preoperative prognostic scoring tools have notable limitations, making it challenging to identify patients who may benefit from neoadjuvant therapy. There is an urgent need for a widely recognized and effective tool to assess postoperative prognosis and guide treatment decisions. This study assessed and compared several widely used indicators, including the Heidelberg prognostic pancreatic cancer (HELPP) score, the Glasgow prognostic score (GPS), the systemic immune-inflammation index (SII), and the neutrophil-lymphocyte ratio (NLR).</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 61 pancreatic cancer patients who underwent radical resection at Zhongshan Hospital of Xiamen University from February 2015 to February 2022. The SII was calculated as (platelets × neutrophils/lymphocytes), and the NLR as (neutrophils/lymphocytes). The preoperative HELPP score was derived from American Society of Anesthesiologists (ASA) classification, carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), C-reactive protein (CRP), albumin, and platelets. The GPS was based on albumin and CRP levels. Optimal cut-off values for the quantitative data were established using Youden's index. Kaplan-Meier method and log-rank tests were used to categorize and group the HELPP scores. Univariate and multivariate survival analyses were conducted to explore the relationship between the HELPP score, GPS, SII, NLR, and postoperative survival of the pancreatic cancer patients. Chi-squared tests were used to compare the clinicopathological data across the prognostic score subgroups. The area under the receiver operating characteristic (ROC) curve (AUC) for each score was evaluated to assess predictive accuracy of 1- and 2-year survival.</p><p><strong>Results: </strong>The optimal cut-off values for the SII and NLR were 675.51 and 2.53, respectively. There were no significant differences in the survival times of the patients with HELPP scores of 1, 2, or 3 points (P>0.05); nor between those with scores of 4 and 5 points (P=0.058). The patients with preoperative HELPP scores of ≤3 points were allocated to the low HELPP score group, while those with scores >3 points were allocated to the high HELPP score group. A HELPP score >3 points, CEA ≥1.48 µg/L, and a tumor diameter >4 cm were found to be independent risk factors affecting postoperative prognosis (P<0.05). The SII, GPS, and NLR were not found to be significantly associated with prognosis. There were no statistically significant differences in the clinicopathological characteristics between the two HELPP score groups (P>0.05). The AUCs for overall survival (OS) for the HELPP score were 0.874 at 1 year and 0.696 at 2 years.</p><p><strong>Conclusions: </strong>The preoperative HELPP score is a promising tool for evaluating prognosis in patients with resectable pancreatic cancer, helpful in developing more appropriate preoperative treatment.</p>\",\"PeriodicalId\":12760,\"journal\":{\"name\":\"Gland surgery\",\"volume\":\"14 6\",\"pages\":\"1112-1127\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12261355/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gland surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/gs-2025-132\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gland surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/gs-2025-132","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
The preoperative HELPP score can be used as a prognostic assessment tool for resectable pancreatic cancer patients, and may be applicable to patients in China as well.
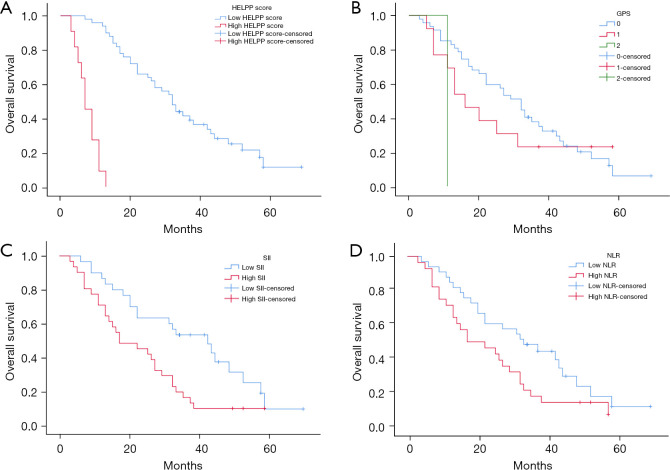
Background: The incidence of pancreatic ductal adenocarcinoma (PDAC) is increasing annually, and the prognosis remains poor. There is currently no consensus on using neoadjuvant therapy for resectable pancreatic cancer. Further, existing preoperative prognostic scoring tools have notable limitations, making it challenging to identify patients who may benefit from neoadjuvant therapy. There is an urgent need for a widely recognized and effective tool to assess postoperative prognosis and guide treatment decisions. This study assessed and compared several widely used indicators, including the Heidelberg prognostic pancreatic cancer (HELPP) score, the Glasgow prognostic score (GPS), the systemic immune-inflammation index (SII), and the neutrophil-lymphocyte ratio (NLR).
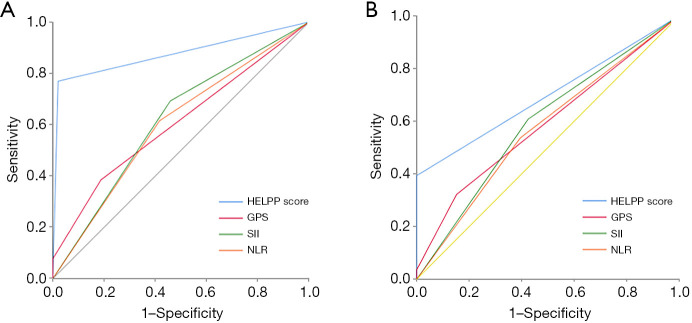
Methods: A retrospective analysis was conducted on 61 pancreatic cancer patients who underwent radical resection at Zhongshan Hospital of Xiamen University from February 2015 to February 2022. The SII was calculated as (platelets × neutrophils/lymphocytes), and the NLR as (neutrophils/lymphocytes). The preoperative HELPP score was derived from American Society of Anesthesiologists (ASA) classification, carbohydrate antigen 19-9 (CA19-9), carcinoembryonic antigen (CEA), C-reactive protein (CRP), albumin, and platelets. The GPS was based on albumin and CRP levels. Optimal cut-off values for the quantitative data were established using Youden's index. Kaplan-Meier method and log-rank tests were used to categorize and group the HELPP scores. Univariate and multivariate survival analyses were conducted to explore the relationship between the HELPP score, GPS, SII, NLR, and postoperative survival of the pancreatic cancer patients. Chi-squared tests were used to compare the clinicopathological data across the prognostic score subgroups. The area under the receiver operating characteristic (ROC) curve (AUC) for each score was evaluated to assess predictive accuracy of 1- and 2-year survival.
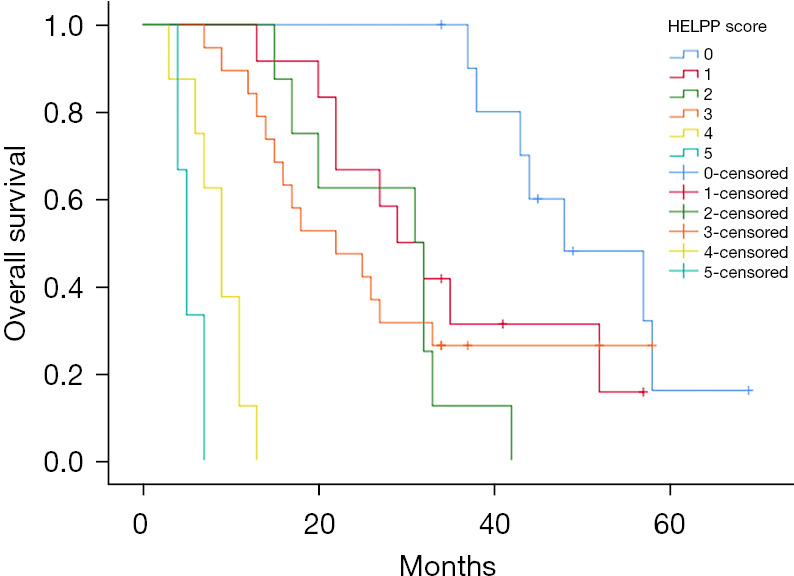
Results: The optimal cut-off values for the SII and NLR were 675.51 and 2.53, respectively. There were no significant differences in the survival times of the patients with HELPP scores of 1, 2, or 3 points (P>0.05); nor between those with scores of 4 and 5 points (P=0.058). The patients with preoperative HELPP scores of ≤3 points were allocated to the low HELPP score group, while those with scores >3 points were allocated to the high HELPP score group. A HELPP score >3 points, CEA ≥1.48 µg/L, and a tumor diameter >4 cm were found to be independent risk factors affecting postoperative prognosis (P<0.05). The SII, GPS, and NLR were not found to be significantly associated with prognosis. There were no statistically significant differences in the clinicopathological characteristics between the two HELPP score groups (P>0.05). The AUCs for overall survival (OS) for the HELPP score were 0.874 at 1 year and 0.696 at 2 years.
Conclusions: The preoperative HELPP score is a promising tool for evaluating prognosis in patients with resectable pancreatic cancer, helpful in developing more appropriate preoperative treatment.
期刊介绍:
Gland Surgery (Gland Surg; GS, Print ISSN 2227-684X; Online ISSN 2227-8575) being indexed by PubMed/PubMed Central, is an open access, peer-review journal launched at May of 2012, published bio-monthly since February 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


