Thomas Grange, Elsa Poullot, Marie Parrens, Alexandra Traverse-Glehen, Charlotte Syrykh, Luc Xerri, Julie Bruneau, Virginie Fataccioli, Nadia Amara, Romain Dubois, Anne Moreau, Alina Nicolae, Fanny Drieux, Vanessa Lacheretz-Szablewski, Francisco Llamas-Gutierrez, Albane Ledoux-Pilon, Marie-Christine Copin, Catherine Chassagne-Clément, François Lemonnier, Pierre Brousset, Philippe Gaulard
{"title":"外周T细胞和nk细胞淋巴瘤实体通过法国淋巴病网络数据库的分布重新评估","authors":"Thomas Grange, Elsa Poullot, Marie Parrens, Alexandra Traverse-Glehen, Charlotte Syrykh, Luc Xerri, Julie Bruneau, Virginie Fataccioli, Nadia Amara, Romain Dubois, Anne Moreau, Alina Nicolae, Fanny Drieux, Vanessa Lacheretz-Szablewski, Francisco Llamas-Gutierrez, Albane Ledoux-Pilon, Marie-Christine Copin, Catherine Chassagne-Clément, François Lemonnier, Pierre Brousset, Philippe Gaulard","doi":"10.1002/hem3.70181","DOIUrl":null,"url":null,"abstract":"<p>The French National Cancer Institute-labelled Lymphopath network was established to provide real-time expert histopathological review of every newly diagnosed or suspected lymphoma in France. It is composed of expert hematopathologists working across 31 academic institutions, equipped with comprehensive access to immunohistochemistry, fluorescent in situ hybridization (FISH), clonality analysis, and molecular testing (Figure 1A). In 2017, we reported<span><sup>1</sup></span> on a review of 36,920 lymphomas registered between 2010 and 2013, including 2049 noncutaneous peripheral T-cell lymphomas (PTCLs). These diagnoses were established according to the criteria of the 2008 WHO classification of lymphoid neoplasms.<span><sup>2</sup></span></p><p>The 2017 revision of the WHO classification<span><sup>3</sup></span> introduced significant changes to the classification of PTCLs, which have been largely upheld in the recently updated WHO and ICC classifications.<span><sup>4, 5</sup></span> An important change was the recognition of a broad umbrella category of PTCLs derived from T follicular helper cells (TFH)—now referred to as (nodal) TFH lymphomas (TFHL)—encompassing angioimmunoblastic T-cell lymphoma (AITL) (TFHL, angioimmunoblastic-type), follicular T-cell lymphoma (TFHL, follicular type), and nodal PTCL with TFH phenotype (TFHL, not otherwise specified [NOS]). The latter were classified as PTCL, NOS prior to the 2017 classification. TFHLs share expression of TFH-related antigens as well as clinical features and recurrent mutations.<span><sup>6, 7</sup></span> Another update was the renaming of enteropathy-associated T-cell lymphoma (EATL) type 2 as monomorphic epitheliotropic intestinal T-cell lymphoma (MEITL) to reflect its distinct pathological, immunophenotypic, genetic, and clinical characteristics and its lack of association with celiac disease.<span><sup>8, 9</sup></span> Additionally, two rare entities, indolent T-cell lymphoproliferative disorder of the gastrointestinal tract and breast implant-associated anaplastic large-cell lymphoma (ALCL), were introduced in the 2017 classification. Our study aims to evaluate how these changes have impacted the relative distribution of noncutaneous PTCLs in France.</p><p>Data from all noncutaneous lymphomas newly diagnosed between January 2018 and December 2021 were extracted from the Lymphopath database in March 2024. All cases had been classified according to the 2017 WHO classification after expert review by the Lymphopath hematopathologists. Among the 44,035 cases registered, 2331 (5.3%) were considered as PTCL by the referral pathologist, whereas 2751 (6.2%) had a final diagnosis of T-cell lymphoma after expert review. T-cell lymphoblastic lymphomas/acute lymphoblastic leukemias (<i>n</i> = 220) were excluded from the analysis, resulting in a total of 2529 noncutaneous PTCLs over the 4-year period (Figure 1B). This represents a 23.4% increase in the annual incidence of PTCL registered by the Lymphopath network compared to our previous report.<span><sup>1</sup></span> While an actual increase in PTCL incidence in France cannot be entirely ruled out, this increase more likely reflects the broader integration of Lymphopath network into clinical practice by both pathologists and clinicians, resulting in a more exhaustive registration of newly diagnosed lymphomas than a decade ago. It is noteworthy that the number of cases registered in 2020 was 5.7% lower than the average of the other 3 years, likely reflecting a decrease in lymphoma diagnosed or registered in the database during the COVID-19 pandemic.</p><p>The median age of patients with PTCL was 68 years, with only 2.1% of children (<18 years, <i>n</i> = 52). There was a slight male predominance (male to female ratio: 1.4:1), consistent with previous reports.<span><sup>10</sup></span> Most diagnoses were based on surgical excisions or biopsies (63.9%, <i>n</i> = 1617), while core needle biopsies only accounted for 34.5% of cases (<i>n</i> = 874), with biopsy type unrecorded in 1.5% of cases (<i>n</i> = 38). In comparison, the distribution of surgical versus core needle biopsies was 51.1% versus 47.1% in B-cell lymphomas. This reflects the inherent challenges of diagnosing and classifying PTCLs using core needle biopsy,<span><sup>11</sup></span> which often require additional immunostainings, in situ hybridization techniques (essentially for EBV), molecular tests (clonality analyses, mutation detection by PCR, or next-generation sequencing [NGS]), or FISH techniques (especially for the DUSP22 rearrangement). These analyses were performed in 92.3%, 50.2%, 39.6%, and 8.6% of cases, respectively, at the expert Lymphopath center. A diagnostic change between the referral and the expert pathologists occurred in 31.6% of patients (<i>n</i> = 798), frequently involving reclassification toward nodal TFH lymphoma (Figure 1C).</p><p>Among the 798 cases with a diagnostic change, 297 (11.7%) had been classified by the referral pathologist as either a different PTCL subtype or an unclassified PTCL. The remaining 501 cases (19.8%) had an initial diagnosis other than PTCL (64 B-cell lymphomas, 72 classic Hodgkin lymphomas, 121 unclassified lymphomas, 3 lymphoblastic T-cell lymphomas, 169 benign lesions, 6 nonhematological malignancies, and 66 without proposed diagnosis). These findings highlight that the diagnosis of PTCL remains challenging for nonexpert pathologists, requiring expertise in lymphoma pathology and often molecular testing performed in approximately 40% of cases in our series, a resource frequently not available in the referral centers. Finally, 4.9% of cases remained unclassified PTCLs, due to poor-quality biopsy samples, which hindered the full range of ancillary techniques necessary for a definitive classification of PTCL. Conversely, among the 2331 cases considered as PTCL by the referral pathologist, 303 (13.0%) had a final diagnosis of another condition, including B-cell lymphoma (4.1%, <i>n</i> = 96), Hodgkin lymphoma (2.0%, <i>n</i> = 47), or benign lesion (2.2%, <i>n</i> = 51), reinforcing the importance of expert review for the diagnosis of PTCL (Supporting Information S1: Table 1 and Supporting Information S1: Figure 1).</p><p>Nodal TFH lymphomas were by far the most prevalent subtype of PTCL comprising 42.7% of cases (<i>n</i> = 1081). These included 36.8% AITL (<i>n</i> = 931), 5.3% TFHL, NOS (<i>n</i> = 133), and 0.7% TFHL, follicular type (<i>n</i> = 17) (Figure 2A and Supporting Information S1: Table 2). ALCL represented 20.5% of cases (<i>n</i> = 518), with a higher prevalence of ALK-negative ALCL (12,7%, <i>n</i> = 321) than ALK-positive ALCL (7.8%, <i>n</i> = 197). Notably, ALK-negative ALCL included 33 cases of breast implant-associated ALCL (1.3%). Consequently, PTCL-NOS only ranked third, accounting for only 15.3% of all noncutaneous PTCLs.</p><p>Mature T-cell and NK-cell leukemias represented 6.4% of cases (<i>n</i> = 163), with the most frequent entities being adult T-cell lymphoma leukemias/lymphomas (2.9%, <i>n</i> = 74) and T-cell large granular lymphocytic leukemia (2.6%, <i>n</i> = 66). This number is likely significantly underestimated, as the Lymphopath database does not include systematically leukemic forms but primarily those diagnosed through biopsies. Intestinal T-cell lymphoma comprised 3.8% (<i>n</i> = 97) of PTCLs, with 1.9% of EATL (<i>n</i> = 47), 1.4% of MEITL (<i>n</i> = 35), 0.4% of intestinal T-cell lymphoma NOS (<i>n</i> = 9), and only six cases (0.2%) of indolent T-cell lymphoproliferative disorder of the gastro-intestinal tract. Extranodal NK/T-cell lymphoma, nasal type represented 5.1% of cases (<i>n</i> = 130). All other entities were rare, each representing less than 0.5% of the total. In particular, over the 4-year study period, only 16 (0.6%) hepatosplenic T-cell lymphomas were recorded in the database.</p><p>As expected, ALK-positive ALCL was the most common entity among young patients, accounting for 77% of PTCLs in individuals younger than 18 years of age and 58% in those younger than 30 years of age (Figure 2B). In contrast, 51% of patients older than 60 years of age were diagnosed with nodal TFH lymphoma.</p><p>Compared with the previous report based on the 2008 WHO classification for the period 2010–2013,<span><sup>1</sup></span> we observed a striking decrease in the prevalence of PTCL-NOS, from 26.9% to 15.3% (Supporting Information S1: Figure 2). This shift parallels an increased proportion of TFH lymphomas (42.7% vs. 36.0%) and ALK-negative ALCL (12.7%, including BIA-ALCL, vs. 7.9%). The increase in TFH lymphomas is mainly driven by the recognition of nodal TFH lymphomas other than AITL, since the 2017 WHO classification, while the frequency of AITL remains remarkably stable (36.8% vs. 36%). Consequently, the overall prevalence of TFH lymphoma is significantly higher than reported in previous studies<span><sup>10, 12-14</sup></span> prior to the changes introduced in recent classifications.<span><sup>3-5</sup></span> While geographical variations influenced by environmental and genetic factors cannot be formally excluded, the observed increase may also reflect enhanced diagnostic precision enabled by broader immunohistochemical markers and molecular testing,<span><sup>7</sup></span> which are often required for the accurate diagnosis of nodal TFH lymphoma.<span><sup>15, 16</sup></span> A key strength of the Lymphopath network is that the expert pathologists have easy access to these ancillary techniques, ensuring diagnostic accuracy.</p><p>ALK-negative ALCL is a clinically and genetically heterogeneous disease. Since the 2008 WHO classification, new clinical or genetic subtypes have been incorporated into the 2017 WHO classification, such as BIA-ALCL. In addition, a subset of ALK-negative ALCL cases harbors <i>DUSP22</i> rearrangements, which are more often associated with the absence of cytotoxic markers and EMA expression, and may be linked to a better prognosis, while a small subset with <i>TP63</i> rearrangements is highly aggressive.<span><sup>17</sup></span> Given that ALK-negative ALCL lacks specific immunohistochemical markers, the detection of these rearrangements by FISH can support the diagnosis and may partially explain the increased incidence of ALK-negative ALCL.</p><p>In conclusion, this study remains highly relevant today, as the WHO and ICC 2022 updated classifications<span><sup>4, 5</sup></span> introduced only minor changes to the 2017 WHO classification of PTCLs. This highlights that TFH lymphoma is by far the most prevalent subtype among noncutaneous PTCLs, accounting for over half the PTCL cases in patients older than 60 years of age. Additionally, it provides new data on the frequency of recently recognized entities, such as MEITL, which appears nearly as common as EATL in France. Advances in lymphomas classification have reduced significantly the proportion of the heterogeneous group of PTCL-NOS, which now represents a minority of PTCLs. Although a molecular subclassification of PTCL-NOS based on gene expression profiling has been proposed,<span><sup>18, 19</sup></span> a better characterization of these subgroups, including their clinical implication, is still needed before they can be integrated into future refined classifications of PTCLs.</p><p><b>Thomas Grange</b>: Conceptualization; writing—original draft; writing—review and editing. <b>Elsa Poullot</b>: Conceptualization; investigation. <b>Marie Parrens</b>: Investigation. <b>Alexandra Traverse-Glehen</b>: Investigation. <b>Charlotte Syrykh</b>: Investigation. <b>Luc Xerri</b>: Investigation. <b>Julie Bruneau</b>: Investigation. <b>Virginie Fataccioli</b>: Data curation; writing—original draft. <b>Nadia Amara</b>: Data curation; writing—original draft. <b>Romain Dubois</b>: Investigation. <b>Anne Moreau</b>: Investigation. <b>Alina Nicolae</b>: Investigation. <b>Fanny Drieux</b>: Investigation. <b>Vanessa Lacheretz-Szablewski</b>: Investigation. <b>Francisco Llamas-Gutierrez</b>: Investigation. <b>Albane Ledoux-Pilon</b>: Investigation. <b>Marie-Christine Copin</b>: Investigation. <b>Catherine Chassagne-Clément</b>: Investigation. <b>François Lemonnier</b>: Conceptualization; writing—original draft; writing—review and editing; supervision. <b>Pierre Brousset</b>: Conceptualization; investigation; writing—review and editing; supervision. <b>Philippe Gaulard</b>: Conceptualization; investigation; writing—original draft; writing—review and editing; supervision.</p><p>Romain Dubois reports consulting for AstraZeneca, Recordati Rare Disease, Owkin, Roche, Kyowa Kirin, and Takeda. Philippe Gaulard reports a consulting or advisory role for Takeda, Gilead, and Recordati; research funding from Innate Pharma, Takeda, and Sanofi; and paid travel to meetings from Roche. François Lemonnier reports honoraria from Takeda and AstraZeneca; advisory board for Miltenyi, Kyowa Kirin and BMS; paid travel from Roche, Gilead, AbbVie, and BeiGene; and research funding from BMS and Roche.</p><p>Ethics approval is not applicable to this study.</p><p>This study was supported by the Institut National du Cancer (INCa), Institut National de la Santé et de la Recherche Médicale (INSERM), the labex TOUCAN, and the Institut Carnot CALYM. The authors have no conflicting financial interests.</p>","PeriodicalId":12982,"journal":{"name":"HemaSphere","volume":"9 7","pages":""},"PeriodicalIF":14.6000,"publicationDate":"2025-07-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.70181","citationCount":"0","resultStr":"{\"title\":\"Distribution reappraisal of peripheral T- and NK-cell lymphoma entities through the French Lymphopath network database\",\"authors\":\"Thomas Grange, Elsa Poullot, Marie Parrens, Alexandra Traverse-Glehen, Charlotte Syrykh, Luc Xerri, Julie Bruneau, Virginie Fataccioli, Nadia Amara, Romain Dubois, Anne Moreau, Alina Nicolae, Fanny Drieux, Vanessa Lacheretz-Szablewski, Francisco Llamas-Gutierrez, Albane Ledoux-Pilon, Marie-Christine Copin, Catherine Chassagne-Clément, François Lemonnier, Pierre Brousset, Philippe Gaulard\",\"doi\":\"10.1002/hem3.70181\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The French National Cancer Institute-labelled Lymphopath network was established to provide real-time expert histopathological review of every newly diagnosed or suspected lymphoma in France. It is composed of expert hematopathologists working across 31 academic institutions, equipped with comprehensive access to immunohistochemistry, fluorescent in situ hybridization (FISH), clonality analysis, and molecular testing (Figure 1A). In 2017, we reported<span><sup>1</sup></span> on a review of 36,920 lymphomas registered between 2010 and 2013, including 2049 noncutaneous peripheral T-cell lymphomas (PTCLs). These diagnoses were established according to the criteria of the 2008 WHO classification of lymphoid neoplasms.<span><sup>2</sup></span></p><p>The 2017 revision of the WHO classification<span><sup>3</sup></span> introduced significant changes to the classification of PTCLs, which have been largely upheld in the recently updated WHO and ICC classifications.<span><sup>4, 5</sup></span> An important change was the recognition of a broad umbrella category of PTCLs derived from T follicular helper cells (TFH)—now referred to as (nodal) TFH lymphomas (TFHL)—encompassing angioimmunoblastic T-cell lymphoma (AITL) (TFHL, angioimmunoblastic-type), follicular T-cell lymphoma (TFHL, follicular type), and nodal PTCL with TFH phenotype (TFHL, not otherwise specified [NOS]). The latter were classified as PTCL, NOS prior to the 2017 classification. TFHLs share expression of TFH-related antigens as well as clinical features and recurrent mutations.<span><sup>6, 7</sup></span> Another update was the renaming of enteropathy-associated T-cell lymphoma (EATL) type 2 as monomorphic epitheliotropic intestinal T-cell lymphoma (MEITL) to reflect its distinct pathological, immunophenotypic, genetic, and clinical characteristics and its lack of association with celiac disease.<span><sup>8, 9</sup></span> Additionally, two rare entities, indolent T-cell lymphoproliferative disorder of the gastrointestinal tract and breast implant-associated anaplastic large-cell lymphoma (ALCL), were introduced in the 2017 classification. Our study aims to evaluate how these changes have impacted the relative distribution of noncutaneous PTCLs in France.</p><p>Data from all noncutaneous lymphomas newly diagnosed between January 2018 and December 2021 were extracted from the Lymphopath database in March 2024. All cases had been classified according to the 2017 WHO classification after expert review by the Lymphopath hematopathologists. Among the 44,035 cases registered, 2331 (5.3%) were considered as PTCL by the referral pathologist, whereas 2751 (6.2%) had a final diagnosis of T-cell lymphoma after expert review. T-cell lymphoblastic lymphomas/acute lymphoblastic leukemias (<i>n</i> = 220) were excluded from the analysis, resulting in a total of 2529 noncutaneous PTCLs over the 4-year period (Figure 1B). This represents a 23.4% increase in the annual incidence of PTCL registered by the Lymphopath network compared to our previous report.<span><sup>1</sup></span> While an actual increase in PTCL incidence in France cannot be entirely ruled out, this increase more likely reflects the broader integration of Lymphopath network into clinical practice by both pathologists and clinicians, resulting in a more exhaustive registration of newly diagnosed lymphomas than a decade ago. It is noteworthy that the number of cases registered in 2020 was 5.7% lower than the average of the other 3 years, likely reflecting a decrease in lymphoma diagnosed or registered in the database during the COVID-19 pandemic.</p><p>The median age of patients with PTCL was 68 years, with only 2.1% of children (<18 years, <i>n</i> = 52). There was a slight male predominance (male to female ratio: 1.4:1), consistent with previous reports.<span><sup>10</sup></span> Most diagnoses were based on surgical excisions or biopsies (63.9%, <i>n</i> = 1617), while core needle biopsies only accounted for 34.5% of cases (<i>n</i> = 874), with biopsy type unrecorded in 1.5% of cases (<i>n</i> = 38). In comparison, the distribution of surgical versus core needle biopsies was 51.1% versus 47.1% in B-cell lymphomas. This reflects the inherent challenges of diagnosing and classifying PTCLs using core needle biopsy,<span><sup>11</sup></span> which often require additional immunostainings, in situ hybridization techniques (essentially for EBV), molecular tests (clonality analyses, mutation detection by PCR, or next-generation sequencing [NGS]), or FISH techniques (especially for the DUSP22 rearrangement). These analyses were performed in 92.3%, 50.2%, 39.6%, and 8.6% of cases, respectively, at the expert Lymphopath center. A diagnostic change between the referral and the expert pathologists occurred in 31.6% of patients (<i>n</i> = 798), frequently involving reclassification toward nodal TFH lymphoma (Figure 1C).</p><p>Among the 798 cases with a diagnostic change, 297 (11.7%) had been classified by the referral pathologist as either a different PTCL subtype or an unclassified PTCL. The remaining 501 cases (19.8%) had an initial diagnosis other than PTCL (64 B-cell lymphomas, 72 classic Hodgkin lymphomas, 121 unclassified lymphomas, 3 lymphoblastic T-cell lymphomas, 169 benign lesions, 6 nonhematological malignancies, and 66 without proposed diagnosis). These findings highlight that the diagnosis of PTCL remains challenging for nonexpert pathologists, requiring expertise in lymphoma pathology and often molecular testing performed in approximately 40% of cases in our series, a resource frequently not available in the referral centers. Finally, 4.9% of cases remained unclassified PTCLs, due to poor-quality biopsy samples, which hindered the full range of ancillary techniques necessary for a definitive classification of PTCL. Conversely, among the 2331 cases considered as PTCL by the referral pathologist, 303 (13.0%) had a final diagnosis of another condition, including B-cell lymphoma (4.1%, <i>n</i> = 96), Hodgkin lymphoma (2.0%, <i>n</i> = 47), or benign lesion (2.2%, <i>n</i> = 51), reinforcing the importance of expert review for the diagnosis of PTCL (Supporting Information S1: Table 1 and Supporting Information S1: Figure 1).</p><p>Nodal TFH lymphomas were by far the most prevalent subtype of PTCL comprising 42.7% of cases (<i>n</i> = 1081). These included 36.8% AITL (<i>n</i> = 931), 5.3% TFHL, NOS (<i>n</i> = 133), and 0.7% TFHL, follicular type (<i>n</i> = 17) (Figure 2A and Supporting Information S1: Table 2). ALCL represented 20.5% of cases (<i>n</i> = 518), with a higher prevalence of ALK-negative ALCL (12,7%, <i>n</i> = 321) than ALK-positive ALCL (7.8%, <i>n</i> = 197). Notably, ALK-negative ALCL included 33 cases of breast implant-associated ALCL (1.3%). Consequently, PTCL-NOS only ranked third, accounting for only 15.3% of all noncutaneous PTCLs.</p><p>Mature T-cell and NK-cell leukemias represented 6.4% of cases (<i>n</i> = 163), with the most frequent entities being adult T-cell lymphoma leukemias/lymphomas (2.9%, <i>n</i> = 74) and T-cell large granular lymphocytic leukemia (2.6%, <i>n</i> = 66). This number is likely significantly underestimated, as the Lymphopath database does not include systematically leukemic forms but primarily those diagnosed through biopsies. Intestinal T-cell lymphoma comprised 3.8% (<i>n</i> = 97) of PTCLs, with 1.9% of EATL (<i>n</i> = 47), 1.4% of MEITL (<i>n</i> = 35), 0.4% of intestinal T-cell lymphoma NOS (<i>n</i> = 9), and only six cases (0.2%) of indolent T-cell lymphoproliferative disorder of the gastro-intestinal tract. Extranodal NK/T-cell lymphoma, nasal type represented 5.1% of cases (<i>n</i> = 130). All other entities were rare, each representing less than 0.5% of the total. In particular, over the 4-year study period, only 16 (0.6%) hepatosplenic T-cell lymphomas were recorded in the database.</p><p>As expected, ALK-positive ALCL was the most common entity among young patients, accounting for 77% of PTCLs in individuals younger than 18 years of age and 58% in those younger than 30 years of age (Figure 2B). In contrast, 51% of patients older than 60 years of age were diagnosed with nodal TFH lymphoma.</p><p>Compared with the previous report based on the 2008 WHO classification for the period 2010–2013,<span><sup>1</sup></span> we observed a striking decrease in the prevalence of PTCL-NOS, from 26.9% to 15.3% (Supporting Information S1: Figure 2). This shift parallels an increased proportion of TFH lymphomas (42.7% vs. 36.0%) and ALK-negative ALCL (12.7%, including BIA-ALCL, vs. 7.9%). The increase in TFH lymphomas is mainly driven by the recognition of nodal TFH lymphomas other than AITL, since the 2017 WHO classification, while the frequency of AITL remains remarkably stable (36.8% vs. 36%). Consequently, the overall prevalence of TFH lymphoma is significantly higher than reported in previous studies<span><sup>10, 12-14</sup></span> prior to the changes introduced in recent classifications.<span><sup>3-5</sup></span> While geographical variations influenced by environmental and genetic factors cannot be formally excluded, the observed increase may also reflect enhanced diagnostic precision enabled by broader immunohistochemical markers and molecular testing,<span><sup>7</sup></span> which are often required for the accurate diagnosis of nodal TFH lymphoma.<span><sup>15, 16</sup></span> A key strength of the Lymphopath network is that the expert pathologists have easy access to these ancillary techniques, ensuring diagnostic accuracy.</p><p>ALK-negative ALCL is a clinically and genetically heterogeneous disease. Since the 2008 WHO classification, new clinical or genetic subtypes have been incorporated into the 2017 WHO classification, such as BIA-ALCL. In addition, a subset of ALK-negative ALCL cases harbors <i>DUSP22</i> rearrangements, which are more often associated with the absence of cytotoxic markers and EMA expression, and may be linked to a better prognosis, while a small subset with <i>TP63</i> rearrangements is highly aggressive.<span><sup>17</sup></span> Given that ALK-negative ALCL lacks specific immunohistochemical markers, the detection of these rearrangements by FISH can support the diagnosis and may partially explain the increased incidence of ALK-negative ALCL.</p><p>In conclusion, this study remains highly relevant today, as the WHO and ICC 2022 updated classifications<span><sup>4, 5</sup></span> introduced only minor changes to the 2017 WHO classification of PTCLs. This highlights that TFH lymphoma is by far the most prevalent subtype among noncutaneous PTCLs, accounting for over half the PTCL cases in patients older than 60 years of age. Additionally, it provides new data on the frequency of recently recognized entities, such as MEITL, which appears nearly as common as EATL in France. Advances in lymphomas classification have reduced significantly the proportion of the heterogeneous group of PTCL-NOS, which now represents a minority of PTCLs. Although a molecular subclassification of PTCL-NOS based on gene expression profiling has been proposed,<span><sup>18, 19</sup></span> a better characterization of these subgroups, including their clinical implication, is still needed before they can be integrated into future refined classifications of PTCLs.</p><p><b>Thomas Grange</b>: Conceptualization; writing—original draft; writing—review and editing. <b>Elsa Poullot</b>: Conceptualization; investigation. <b>Marie Parrens</b>: Investigation. <b>Alexandra Traverse-Glehen</b>: Investigation. <b>Charlotte Syrykh</b>: Investigation. <b>Luc Xerri</b>: Investigation. <b>Julie Bruneau</b>: Investigation. <b>Virginie Fataccioli</b>: Data curation; writing—original draft. <b>Nadia Amara</b>: Data curation; writing—original draft. <b>Romain Dubois</b>: Investigation. <b>Anne Moreau</b>: Investigation. <b>Alina Nicolae</b>: Investigation. <b>Fanny Drieux</b>: Investigation. <b>Vanessa Lacheretz-Szablewski</b>: Investigation. <b>Francisco Llamas-Gutierrez</b>: Investigation. <b>Albane Ledoux-Pilon</b>: Investigation. <b>Marie-Christine Copin</b>: Investigation. <b>Catherine Chassagne-Clément</b>: Investigation. <b>François Lemonnier</b>: Conceptualization; writing—original draft; writing—review and editing; supervision. <b>Pierre Brousset</b>: Conceptualization; investigation; writing—review and editing; supervision. <b>Philippe Gaulard</b>: Conceptualization; investigation; writing—original draft; writing—review and editing; supervision.</p><p>Romain Dubois reports consulting for AstraZeneca, Recordati Rare Disease, Owkin, Roche, Kyowa Kirin, and Takeda. Philippe Gaulard reports a consulting or advisory role for Takeda, Gilead, and Recordati; research funding from Innate Pharma, Takeda, and Sanofi; and paid travel to meetings from Roche. François Lemonnier reports honoraria from Takeda and AstraZeneca; advisory board for Miltenyi, Kyowa Kirin and BMS; paid travel from Roche, Gilead, AbbVie, and BeiGene; and research funding from BMS and Roche.</p><p>Ethics approval is not applicable to this study.</p><p>This study was supported by the Institut National du Cancer (INCa), Institut National de la Santé et de la Recherche Médicale (INSERM), the labex TOUCAN, and the Institut Carnot CALYM. The authors have no conflicting financial interests.</p>\",\"PeriodicalId\":12982,\"journal\":{\"name\":\"HemaSphere\",\"volume\":\"9 7\",\"pages\":\"\"},\"PeriodicalIF\":14.6000,\"publicationDate\":\"2025-07-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hem3.70181\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"HemaSphere\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70181\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"HemaSphere","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hem3.70181","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Distribution reappraisal of peripheral T- and NK-cell lymphoma entities through the French Lymphopath network database
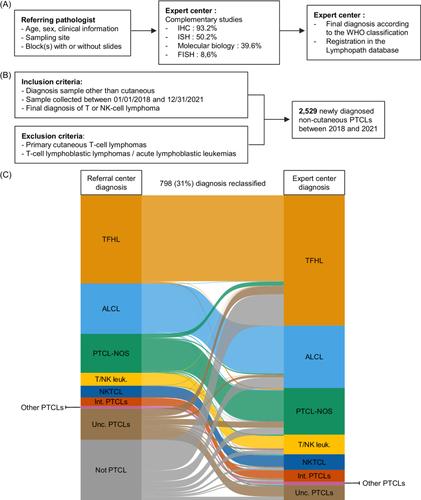
The French National Cancer Institute-labelled Lymphopath network was established to provide real-time expert histopathological review of every newly diagnosed or suspected lymphoma in France. It is composed of expert hematopathologists working across 31 academic institutions, equipped with comprehensive access to immunohistochemistry, fluorescent in situ hybridization (FISH), clonality analysis, and molecular testing (Figure 1A). In 2017, we reported1 on a review of 36,920 lymphomas registered between 2010 and 2013, including 2049 noncutaneous peripheral T-cell lymphomas (PTCLs). These diagnoses were established according to the criteria of the 2008 WHO classification of lymphoid neoplasms.2
The 2017 revision of the WHO classification3 introduced significant changes to the classification of PTCLs, which have been largely upheld in the recently updated WHO and ICC classifications.4, 5 An important change was the recognition of a broad umbrella category of PTCLs derived from T follicular helper cells (TFH)—now referred to as (nodal) TFH lymphomas (TFHL)—encompassing angioimmunoblastic T-cell lymphoma (AITL) (TFHL, angioimmunoblastic-type), follicular T-cell lymphoma (TFHL, follicular type), and nodal PTCL with TFH phenotype (TFHL, not otherwise specified [NOS]). The latter were classified as PTCL, NOS prior to the 2017 classification. TFHLs share expression of TFH-related antigens as well as clinical features and recurrent mutations.6, 7 Another update was the renaming of enteropathy-associated T-cell lymphoma (EATL) type 2 as monomorphic epitheliotropic intestinal T-cell lymphoma (MEITL) to reflect its distinct pathological, immunophenotypic, genetic, and clinical characteristics and its lack of association with celiac disease.8, 9 Additionally, two rare entities, indolent T-cell lymphoproliferative disorder of the gastrointestinal tract and breast implant-associated anaplastic large-cell lymphoma (ALCL), were introduced in the 2017 classification. Our study aims to evaluate how these changes have impacted the relative distribution of noncutaneous PTCLs in France.
Data from all noncutaneous lymphomas newly diagnosed between January 2018 and December 2021 were extracted from the Lymphopath database in March 2024. All cases had been classified according to the 2017 WHO classification after expert review by the Lymphopath hematopathologists. Among the 44,035 cases registered, 2331 (5.3%) were considered as PTCL by the referral pathologist, whereas 2751 (6.2%) had a final diagnosis of T-cell lymphoma after expert review. T-cell lymphoblastic lymphomas/acute lymphoblastic leukemias (n = 220) were excluded from the analysis, resulting in a total of 2529 noncutaneous PTCLs over the 4-year period (Figure 1B). This represents a 23.4% increase in the annual incidence of PTCL registered by the Lymphopath network compared to our previous report.1 While an actual increase in PTCL incidence in France cannot be entirely ruled out, this increase more likely reflects the broader integration of Lymphopath network into clinical practice by both pathologists and clinicians, resulting in a more exhaustive registration of newly diagnosed lymphomas than a decade ago. It is noteworthy that the number of cases registered in 2020 was 5.7% lower than the average of the other 3 years, likely reflecting a decrease in lymphoma diagnosed or registered in the database during the COVID-19 pandemic.
The median age of patients with PTCL was 68 years, with only 2.1% of children (<18 years, n = 52). There was a slight male predominance (male to female ratio: 1.4:1), consistent with previous reports.10 Most diagnoses were based on surgical excisions or biopsies (63.9%, n = 1617), while core needle biopsies only accounted for 34.5% of cases (n = 874), with biopsy type unrecorded in 1.5% of cases (n = 38). In comparison, the distribution of surgical versus core needle biopsies was 51.1% versus 47.1% in B-cell lymphomas. This reflects the inherent challenges of diagnosing and classifying PTCLs using core needle biopsy,11 which often require additional immunostainings, in situ hybridization techniques (essentially for EBV), molecular tests (clonality analyses, mutation detection by PCR, or next-generation sequencing [NGS]), or FISH techniques (especially for the DUSP22 rearrangement). These analyses were performed in 92.3%, 50.2%, 39.6%, and 8.6% of cases, respectively, at the expert Lymphopath center. A diagnostic change between the referral and the expert pathologists occurred in 31.6% of patients (n = 798), frequently involving reclassification toward nodal TFH lymphoma (Figure 1C).
Among the 798 cases with a diagnostic change, 297 (11.7%) had been classified by the referral pathologist as either a different PTCL subtype or an unclassified PTCL. The remaining 501 cases (19.8%) had an initial diagnosis other than PTCL (64 B-cell lymphomas, 72 classic Hodgkin lymphomas, 121 unclassified lymphomas, 3 lymphoblastic T-cell lymphomas, 169 benign lesions, 6 nonhematological malignancies, and 66 without proposed diagnosis). These findings highlight that the diagnosis of PTCL remains challenging for nonexpert pathologists, requiring expertise in lymphoma pathology and often molecular testing performed in approximately 40% of cases in our series, a resource frequently not available in the referral centers. Finally, 4.9% of cases remained unclassified PTCLs, due to poor-quality biopsy samples, which hindered the full range of ancillary techniques necessary for a definitive classification of PTCL. Conversely, among the 2331 cases considered as PTCL by the referral pathologist, 303 (13.0%) had a final diagnosis of another condition, including B-cell lymphoma (4.1%, n = 96), Hodgkin lymphoma (2.0%, n = 47), or benign lesion (2.2%, n = 51), reinforcing the importance of expert review for the diagnosis of PTCL (Supporting Information S1: Table 1 and Supporting Information S1: Figure 1).
Nodal TFH lymphomas were by far the most prevalent subtype of PTCL comprising 42.7% of cases (n = 1081). These included 36.8% AITL (n = 931), 5.3% TFHL, NOS (n = 133), and 0.7% TFHL, follicular type (n = 17) (Figure 2A and Supporting Information S1: Table 2). ALCL represented 20.5% of cases (n = 518), with a higher prevalence of ALK-negative ALCL (12,7%, n = 321) than ALK-positive ALCL (7.8%, n = 197). Notably, ALK-negative ALCL included 33 cases of breast implant-associated ALCL (1.3%). Consequently, PTCL-NOS only ranked third, accounting for only 15.3% of all noncutaneous PTCLs.
Mature T-cell and NK-cell leukemias represented 6.4% of cases (n = 163), with the most frequent entities being adult T-cell lymphoma leukemias/lymphomas (2.9%, n = 74) and T-cell large granular lymphocytic leukemia (2.6%, n = 66). This number is likely significantly underestimated, as the Lymphopath database does not include systematically leukemic forms but primarily those diagnosed through biopsies. Intestinal T-cell lymphoma comprised 3.8% (n = 97) of PTCLs, with 1.9% of EATL (n = 47), 1.4% of MEITL (n = 35), 0.4% of intestinal T-cell lymphoma NOS (n = 9), and only six cases (0.2%) of indolent T-cell lymphoproliferative disorder of the gastro-intestinal tract. Extranodal NK/T-cell lymphoma, nasal type represented 5.1% of cases (n = 130). All other entities were rare, each representing less than 0.5% of the total. In particular, over the 4-year study period, only 16 (0.6%) hepatosplenic T-cell lymphomas were recorded in the database.
As expected, ALK-positive ALCL was the most common entity among young patients, accounting for 77% of PTCLs in individuals younger than 18 years of age and 58% in those younger than 30 years of age (Figure 2B). In contrast, 51% of patients older than 60 years of age were diagnosed with nodal TFH lymphoma.
Compared with the previous report based on the 2008 WHO classification for the period 2010–2013,1 we observed a striking decrease in the prevalence of PTCL-NOS, from 26.9% to 15.3% (Supporting Information S1: Figure 2). This shift parallels an increased proportion of TFH lymphomas (42.7% vs. 36.0%) and ALK-negative ALCL (12.7%, including BIA-ALCL, vs. 7.9%). The increase in TFH lymphomas is mainly driven by the recognition of nodal TFH lymphomas other than AITL, since the 2017 WHO classification, while the frequency of AITL remains remarkably stable (36.8% vs. 36%). Consequently, the overall prevalence of TFH lymphoma is significantly higher than reported in previous studies10, 12-14 prior to the changes introduced in recent classifications.3-5 While geographical variations influenced by environmental and genetic factors cannot be formally excluded, the observed increase may also reflect enhanced diagnostic precision enabled by broader immunohistochemical markers and molecular testing,7 which are often required for the accurate diagnosis of nodal TFH lymphoma.15, 16 A key strength of the Lymphopath network is that the expert pathologists have easy access to these ancillary techniques, ensuring diagnostic accuracy.
ALK-negative ALCL is a clinically and genetically heterogeneous disease. Since the 2008 WHO classification, new clinical or genetic subtypes have been incorporated into the 2017 WHO classification, such as BIA-ALCL. In addition, a subset of ALK-negative ALCL cases harbors DUSP22 rearrangements, which are more often associated with the absence of cytotoxic markers and EMA expression, and may be linked to a better prognosis, while a small subset with TP63 rearrangements is highly aggressive.17 Given that ALK-negative ALCL lacks specific immunohistochemical markers, the detection of these rearrangements by FISH can support the diagnosis and may partially explain the increased incidence of ALK-negative ALCL.
In conclusion, this study remains highly relevant today, as the WHO and ICC 2022 updated classifications4, 5 introduced only minor changes to the 2017 WHO classification of PTCLs. This highlights that TFH lymphoma is by far the most prevalent subtype among noncutaneous PTCLs, accounting for over half the PTCL cases in patients older than 60 years of age. Additionally, it provides new data on the frequency of recently recognized entities, such as MEITL, which appears nearly as common as EATL in France. Advances in lymphomas classification have reduced significantly the proportion of the heterogeneous group of PTCL-NOS, which now represents a minority of PTCLs. Although a molecular subclassification of PTCL-NOS based on gene expression profiling has been proposed,18, 19 a better characterization of these subgroups, including their clinical implication, is still needed before they can be integrated into future refined classifications of PTCLs.
Thomas Grange: Conceptualization; writing—original draft; writing—review and editing. Elsa Poullot: Conceptualization; investigation. Marie Parrens: Investigation. Alexandra Traverse-Glehen: Investigation. Charlotte Syrykh: Investigation. Luc Xerri: Investigation. Julie Bruneau: Investigation. Virginie Fataccioli: Data curation; writing—original draft. Nadia Amara: Data curation; writing—original draft. Romain Dubois: Investigation. Anne Moreau: Investigation. Alina Nicolae: Investigation. Fanny Drieux: Investigation. Vanessa Lacheretz-Szablewski: Investigation. Francisco Llamas-Gutierrez: Investigation. Albane Ledoux-Pilon: Investigation. Marie-Christine Copin: Investigation. Catherine Chassagne-Clément: Investigation. François Lemonnier: Conceptualization; writing—original draft; writing—review and editing; supervision. Pierre Brousset: Conceptualization; investigation; writing—review and editing; supervision. Philippe Gaulard: Conceptualization; investigation; writing—original draft; writing—review and editing; supervision.
Romain Dubois reports consulting for AstraZeneca, Recordati Rare Disease, Owkin, Roche, Kyowa Kirin, and Takeda. Philippe Gaulard reports a consulting or advisory role for Takeda, Gilead, and Recordati; research funding from Innate Pharma, Takeda, and Sanofi; and paid travel to meetings from Roche. François Lemonnier reports honoraria from Takeda and AstraZeneca; advisory board for Miltenyi, Kyowa Kirin and BMS; paid travel from Roche, Gilead, AbbVie, and BeiGene; and research funding from BMS and Roche.
Ethics approval is not applicable to this study.
This study was supported by the Institut National du Cancer (INCa), Institut National de la Santé et de la Recherche Médicale (INSERM), the labex TOUCAN, and the Institut Carnot CALYM. The authors have no conflicting financial interests.
期刊介绍:
HemaSphere, as a publication, is dedicated to disseminating the outcomes of profoundly pertinent basic, translational, and clinical research endeavors within the field of hematology. The journal actively seeks robust studies that unveil novel discoveries with significant ramifications for hematology.
In addition to original research, HemaSphere features review articles and guideline articles that furnish lucid synopses and discussions of emerging developments, along with recommendations for patient care.
Positioned as the foremost resource in hematology, HemaSphere augments its offerings with specialized sections like HemaTopics and HemaPolicy. These segments engender insightful dialogues covering a spectrum of hematology-related topics, including digestible summaries of pivotal articles, updates on new therapies, deliberations on European policy matters, and other noteworthy news items within the field. Steering the course of HemaSphere are Editor in Chief Jan Cools and Deputy Editor in Chief Claire Harrison, alongside the guidance of an esteemed Editorial Board comprising international luminaries in both research and clinical realms, each representing diverse areas of hematologic expertise.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


