Emma Forsgren, Caroline Feldthusen, Sara Wallström, Ida Björkman, Jana Bergholtz, Febe Friberg, Joakim Öhlén
{"title":"从实施以人为本的护理中学习:与哥德堡框架有关的研究的综合。","authors":"Emma Forsgren, Caroline Feldthusen, Sara Wallström, Ida Björkman, Jana Bergholtz, Febe Friberg, Joakim Öhlén","doi":"10.3389/frhs.2025.1589502","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>While research has shown promising effects of person-centred care (PCC) in a variety of settings, it remains to be systematically implemented in practice. Publications exist on conceptual frameworks for PCC implementation, as well as identified barriers and enablers, but a comprehensive overview of lessons learned from PCC implementation efforts is lacking. The aim of this study therefore is to synthesize research-based empirical knowledge on implementation of PCC using the theoretical foundation of the Gothenburg framework.</p><p><strong>Method: </strong>Interpretive meta-synthesis, using the theoretical framing of the Gothenburg framework for PCC, and implementation science in the context of healthcare services in Sweden.</p><p><strong>Results: </strong>The results illuminate that PCC implementation includes three interrelated categories of strategies, more precisely: strategies connected towards creating and safeguarding a person-centred work and care culture, strategies in connection to leaders and change agents, and strategies focused on learning activities and adaption to setting. An ideal of co-creation in partnership is prominent, and both top-down approaches (such as policy) as well as bottom-up approaches (activities/methodologies/tactics) created within services are at play. Implementation strategies are both deliberate and emergent during the implementation process.</p><p><strong>Discussion: </strong>The synthesis connects to available implementation research in that it highlights the importance of care culture, connected leadership at different levels, and learning activities. While patients and family carers are included as partners in intervention research, their role as leaders and actors for change in implementation efforts is not explicitly described.</p><p><strong>Conclusion: </strong>The combination of deliberate and emergent strategies, movements from top-down and bottom-up in combination with the ideal of co-creation at all levels demonstrates the complexities and iterative nature of PCC implementation. By illustrating this complexity and providing examples of handling practical issues, this study contributes to deeper insights on PCC implementation.</p>","PeriodicalId":73088,"journal":{"name":"Frontiers in health services","volume":"5 ","pages":"1589502"},"PeriodicalIF":2.7000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12259557/pdf/","citationCount":"0","resultStr":"{\"title\":\"Learning from the implementation of person-centred care: a meta-synthesis of research related to the Gothenburg framework.\",\"authors\":\"Emma Forsgren, Caroline Feldthusen, Sara Wallström, Ida Björkman, Jana Bergholtz, Febe Friberg, Joakim Öhlén\",\"doi\":\"10.3389/frhs.2025.1589502\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>While research has shown promising effects of person-centred care (PCC) in a variety of settings, it remains to be systematically implemented in practice. Publications exist on conceptual frameworks for PCC implementation, as well as identified barriers and enablers, but a comprehensive overview of lessons learned from PCC implementation efforts is lacking. The aim of this study therefore is to synthesize research-based empirical knowledge on implementation of PCC using the theoretical foundation of the Gothenburg framework.</p><p><strong>Method: </strong>Interpretive meta-synthesis, using the theoretical framing of the Gothenburg framework for PCC, and implementation science in the context of healthcare services in Sweden.</p><p><strong>Results: </strong>The results illuminate that PCC implementation includes three interrelated categories of strategies, more precisely: strategies connected towards creating and safeguarding a person-centred work and care culture, strategies in connection to leaders and change agents, and strategies focused on learning activities and adaption to setting. An ideal of co-creation in partnership is prominent, and both top-down approaches (such as policy) as well as bottom-up approaches (activities/methodologies/tactics) created within services are at play. Implementation strategies are both deliberate and emergent during the implementation process.</p><p><strong>Discussion: </strong>The synthesis connects to available implementation research in that it highlights the importance of care culture, connected leadership at different levels, and learning activities. While patients and family carers are included as partners in intervention research, their role as leaders and actors for change in implementation efforts is not explicitly described.</p><p><strong>Conclusion: </strong>The combination of deliberate and emergent strategies, movements from top-down and bottom-up in combination with the ideal of co-creation at all levels demonstrates the complexities and iterative nature of PCC implementation. By illustrating this complexity and providing examples of handling practical issues, this study contributes to deeper insights on PCC implementation.</p>\",\"PeriodicalId\":73088,\"journal\":{\"name\":\"Frontiers in health services\",\"volume\":\"5 \",\"pages\":\"1589502\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12259557/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in health services\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/frhs.2025.1589502\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in health services","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/frhs.2025.1589502","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Learning from the implementation of person-centred care: a meta-synthesis of research related to the Gothenburg framework.
Introduction: While research has shown promising effects of person-centred care (PCC) in a variety of settings, it remains to be systematically implemented in practice. Publications exist on conceptual frameworks for PCC implementation, as well as identified barriers and enablers, but a comprehensive overview of lessons learned from PCC implementation efforts is lacking. The aim of this study therefore is to synthesize research-based empirical knowledge on implementation of PCC using the theoretical foundation of the Gothenburg framework.
Method: Interpretive meta-synthesis, using the theoretical framing of the Gothenburg framework for PCC, and implementation science in the context of healthcare services in Sweden.
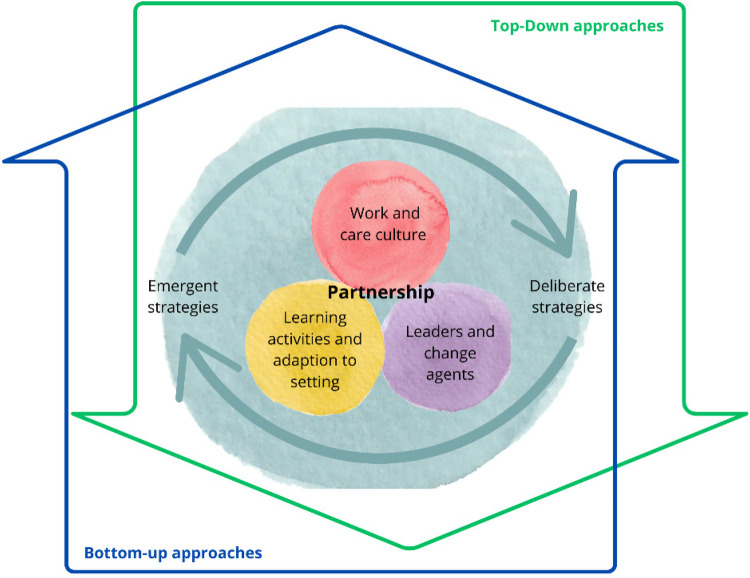
Results: The results illuminate that PCC implementation includes three interrelated categories of strategies, more precisely: strategies connected towards creating and safeguarding a person-centred work and care culture, strategies in connection to leaders and change agents, and strategies focused on learning activities and adaption to setting. An ideal of co-creation in partnership is prominent, and both top-down approaches (such as policy) as well as bottom-up approaches (activities/methodologies/tactics) created within services are at play. Implementation strategies are both deliberate and emergent during the implementation process.
Discussion: The synthesis connects to available implementation research in that it highlights the importance of care culture, connected leadership at different levels, and learning activities. While patients and family carers are included as partners in intervention research, their role as leaders and actors for change in implementation efforts is not explicitly described.
Conclusion: The combination of deliberate and emergent strategies, movements from top-down and bottom-up in combination with the ideal of co-creation at all levels demonstrates the complexities and iterative nature of PCC implementation. By illustrating this complexity and providing examples of handling practical issues, this study contributes to deeper insights on PCC implementation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


