Kai Tai Derek Yeung, Roumaysaa Bouyardan, Desmond Barton, David Nicol, Sacheen Kumar, Ricky Harminder Bhogal
{"title":"多学科多脏器切除涉及上消化道:英国三级癌症中心的经验。","authors":"Kai Tai Derek Yeung, Roumaysaa Bouyardan, Desmond Barton, David Nicol, Sacheen Kumar, Ricky Harminder Bhogal","doi":"10.1007/s00423-025-03815-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Multivisceral surgical resections (MVR) are highly specialised procedures involving multidisciplinary surgical teams. MVR can be performed to achieve a complete oncological resection of tumours or to achieve cytoreductive surgery. The aim of the study is to evaluate the peri-operative outcomes of patients undergoing oncological multivisceral or multi-tissue resection which involved concomitant resection of the upper digestive tract/organs (oesophagogastric and hepatopancreatic-biliary).</p><p><strong>Methods: </strong>This is a retrospective cohort study of patients treated between May 2019 to May 2023 at the Royal Marsden Hospital, London, United Kingdom. All treatment decisions were ratified at tumour specific multidisciplinary team meetings (MDT).</p><p><strong>Results: </strong>A total of twenty-two patients were included in this series. The mean age and BMI were 56.2 years and 26.5 kg/m<sup>2</sup> respectively. 86% of patients had ASA Grade II and 91% had WHO performance status of zero or one. 59% of patients underwent some form of tumour specific neoadjuvant treatment prior to surgical resection. The indication for surgery was due to malignancies originating from the upper digestive tract (41%), gynaecological organs (32%) and urinary tract (22%). The majority of cases (68%) involved surgeons from two sperate surgical specialties. 91% of cases involved resection of at least three or more organs or soft tissue groups. The mean critical care length of stay and total length of hospital stay was 2.9 days and 17.8 days respectively. 41% patients required inpatient blood transfusion. Clavien-Dindo Grade II, III and IV complication rates were 68%, 14% and 0% respectively. There were no 30-day re-admissions and no 90-day mortalities. The mean duration of follow up was 23.7 months. At time of analysis, the median overall survival (OS) was 21.0 months.</p><p><strong>Conclusions: </strong>Complex MVR can be performed safely with acceptable perioperative outcomes at specialist high-volume centres. To achieve these outcomes patients should be selected carefully on a case-by-case basis with discussion at all respective tumour specific MDTs.</p>","PeriodicalId":17983,"journal":{"name":"Langenbeck's Archives of Surgery","volume":"410 1","pages":"224"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12267298/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multidisciplinary multivisceral resections involving the upper digestive tract: a United Kingdom tertiary cancer centre experience.\",\"authors\":\"Kai Tai Derek Yeung, Roumaysaa Bouyardan, Desmond Barton, David Nicol, Sacheen Kumar, Ricky Harminder Bhogal\",\"doi\":\"10.1007/s00423-025-03815-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Multivisceral surgical resections (MVR) are highly specialised procedures involving multidisciplinary surgical teams. MVR can be performed to achieve a complete oncological resection of tumours or to achieve cytoreductive surgery. The aim of the study is to evaluate the peri-operative outcomes of patients undergoing oncological multivisceral or multi-tissue resection which involved concomitant resection of the upper digestive tract/organs (oesophagogastric and hepatopancreatic-biliary).</p><p><strong>Methods: </strong>This is a retrospective cohort study of patients treated between May 2019 to May 2023 at the Royal Marsden Hospital, London, United Kingdom. All treatment decisions were ratified at tumour specific multidisciplinary team meetings (MDT).</p><p><strong>Results: </strong>A total of twenty-two patients were included in this series. The mean age and BMI were 56.2 years and 26.5 kg/m<sup>2</sup> respectively. 86% of patients had ASA Grade II and 91% had WHO performance status of zero or one. 59% of patients underwent some form of tumour specific neoadjuvant treatment prior to surgical resection. The indication for surgery was due to malignancies originating from the upper digestive tract (41%), gynaecological organs (32%) and urinary tract (22%). The majority of cases (68%) involved surgeons from two sperate surgical specialties. 91% of cases involved resection of at least three or more organs or soft tissue groups. The mean critical care length of stay and total length of hospital stay was 2.9 days and 17.8 days respectively. 41% patients required inpatient blood transfusion. Clavien-Dindo Grade II, III and IV complication rates were 68%, 14% and 0% respectively. There were no 30-day re-admissions and no 90-day mortalities. The mean duration of follow up was 23.7 months. At time of analysis, the median overall survival (OS) was 21.0 months.</p><p><strong>Conclusions: </strong>Complex MVR can be performed safely with acceptable perioperative outcomes at specialist high-volume centres. To achieve these outcomes patients should be selected carefully on a case-by-case basis with discussion at all respective tumour specific MDTs.</p>\",\"PeriodicalId\":17983,\"journal\":{\"name\":\"Langenbeck's Archives of Surgery\",\"volume\":\"410 1\",\"pages\":\"224\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-07-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12267298/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Langenbeck's Archives of Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00423-025-03815-4\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Langenbeck's Archives of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00423-025-03815-4","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Multidisciplinary multivisceral resections involving the upper digestive tract: a United Kingdom tertiary cancer centre experience.
Purpose: Multivisceral surgical resections (MVR) are highly specialised procedures involving multidisciplinary surgical teams. MVR can be performed to achieve a complete oncological resection of tumours or to achieve cytoreductive surgery. The aim of the study is to evaluate the peri-operative outcomes of patients undergoing oncological multivisceral or multi-tissue resection which involved concomitant resection of the upper digestive tract/organs (oesophagogastric and hepatopancreatic-biliary).
Methods: This is a retrospective cohort study of patients treated between May 2019 to May 2023 at the Royal Marsden Hospital, London, United Kingdom. All treatment decisions were ratified at tumour specific multidisciplinary team meetings (MDT).
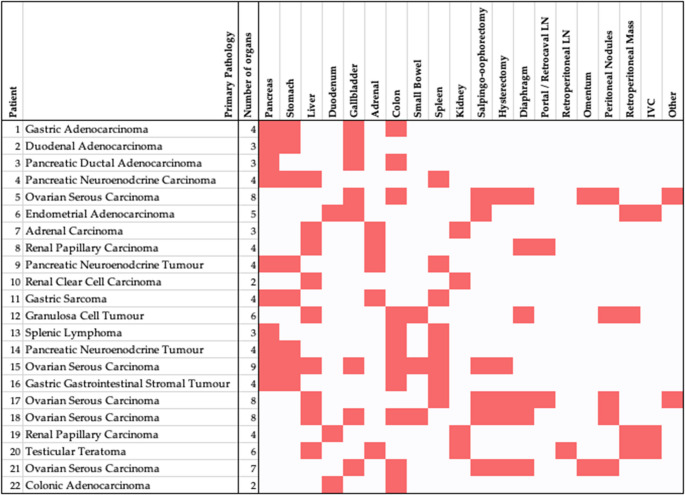
Results: A total of twenty-two patients were included in this series. The mean age and BMI were 56.2 years and 26.5 kg/m2 respectively. 86% of patients had ASA Grade II and 91% had WHO performance status of zero or one. 59% of patients underwent some form of tumour specific neoadjuvant treatment prior to surgical resection. The indication for surgery was due to malignancies originating from the upper digestive tract (41%), gynaecological organs (32%) and urinary tract (22%). The majority of cases (68%) involved surgeons from two sperate surgical specialties. 91% of cases involved resection of at least three or more organs or soft tissue groups. The mean critical care length of stay and total length of hospital stay was 2.9 days and 17.8 days respectively. 41% patients required inpatient blood transfusion. Clavien-Dindo Grade II, III and IV complication rates were 68%, 14% and 0% respectively. There were no 30-day re-admissions and no 90-day mortalities. The mean duration of follow up was 23.7 months. At time of analysis, the median overall survival (OS) was 21.0 months.
Conclusions: Complex MVR can be performed safely with acceptable perioperative outcomes at specialist high-volume centres. To achieve these outcomes patients should be selected carefully on a case-by-case basis with discussion at all respective tumour specific MDTs.
期刊介绍:
Langenbeck''s Archives of Surgery aims to publish the best results in the field of clinical surgery and basic surgical research. The main focus is on providing the highest level of clinical research and clinically relevant basic research. The journal, published exclusively in English, will provide an international discussion forum for the controlled results of clinical surgery. The majority of published contributions will be original articles reporting on clinical data from general and visceral surgery, while endocrine surgery will also be covered. Papers on basic surgical principles from the fields of traumatology, vascular and thoracic surgery are also welcome. Evidence-based medicine is an important criterion for the acceptance of papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


