{"title":"分诊时主诉与72小时死亡率和重症监护入院的关系。","authors":"Niraj Rauniyar, Ankit Kumar Sahu, Bharath Gopinath, Akshay Kumar, Nayer Jamshed, Meera Ekka, Prakash Ranjan Mishra, Sanjeev Bhoi, Tej Prakash Sinha, Gaurav Rajwanshi","doi":"10.4103/jets.jets_127_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Triage is a critical process in prioritizing patients based on acuity to ensure timely care. Patients arrive at the emergency department (ED) with complaints, not diagnoses. High-risk patients are identified based on history, vital signs, mechanism of injury in trauma, and clinical findings. Chief complaints in the ED may suggest acuity independent of other clinical parameters. The objective of this study was to identify high-risk chief complaints associated with intensive care unit (ICU) admission or mortality within 72 h of ED presentation. We also characterized the chief complaints by frequency and evaluated the accuracy of the All India Institute of Medical Sciences Triage Protocol (ATP) in conjunction with high-risk complaints for predicting mortality.</p><p><strong>Methods: </strong>This prospective observational study was conducted at AIIMS, New Delhi, from March 2021 to October 2023, including 1225 patients. Inclusion criteria covered all patients older than 16 years presenting to the ED, excluding cardiac arrest cases, pregnancy-related complications, and individuals declared dead on arrival. Data were collected using predesigned proformas. Univariate and multivariate logistic regression analyses identified high-risk chief complaints.</p><p><strong>Results: </strong>Of the 1754 patients screened, 1225 were included in the analysis. Thirty-four complaints were identified, with six deemed high risk. Specific complaints such as shortness of breath (odds ratio [OR] 43.691, 95% confidence interval [CI] 20.033-95.291, <i>P</i> = 0.001), altered mental status (OR: 6.243, 95% CI: 3.282-11.876, <i>P</i> < 0.001), hematemesis (OR: 3.88, 95% CI: 2.019-7.454, <i>P</i> < 0.001), fall from height (OR: 3.875, 95% CI: 1.874-8.014, <i>P</i> < 0.001), weakness of one side (OR: 3.159, 95% CI: 1.656-6.024, <i>P</i> < 0.001), and chest pain (OR: 1.784, 95% CI: 1.22-3.209, <i>P</i> = 0.043) were significantly associated with adverse outcomes (mortality or ICU admission) at 72 h, even after adjusting for age, gender, and comorbidities. Incorporating high-risk complaints into the ATP triage system increased predictive value (OR 3.12 vs. 7.14).</p><p><strong>Conclusion: </strong>Our findings highlight specific chief complaints as valuable indicators for the early identification of patients at risk of 72-h mortality or ICU admission in the ED. Early identification of high-risk patients can enhance early resuscitation, timely referral to higher-level care, and improve patient outcomes.</p>","PeriodicalId":15692,"journal":{"name":"Journal of Emergencies, Trauma, and Shock","volume":"18 2","pages":"62-68"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12258527/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of Presenting Complaint at Triage with 72-h Mortality and Intensive Care Admission.\",\"authors\":\"Niraj Rauniyar, Ankit Kumar Sahu, Bharath Gopinath, Akshay Kumar, Nayer Jamshed, Meera Ekka, Prakash Ranjan Mishra, Sanjeev Bhoi, Tej Prakash Sinha, Gaurav Rajwanshi\",\"doi\":\"10.4103/jets.jets_127_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Triage is a critical process in prioritizing patients based on acuity to ensure timely care. Patients arrive at the emergency department (ED) with complaints, not diagnoses. High-risk patients are identified based on history, vital signs, mechanism of injury in trauma, and clinical findings. Chief complaints in the ED may suggest acuity independent of other clinical parameters. The objective of this study was to identify high-risk chief complaints associated with intensive care unit (ICU) admission or mortality within 72 h of ED presentation. We also characterized the chief complaints by frequency and evaluated the accuracy of the All India Institute of Medical Sciences Triage Protocol (ATP) in conjunction with high-risk complaints for predicting mortality.</p><p><strong>Methods: </strong>This prospective observational study was conducted at AIIMS, New Delhi, from March 2021 to October 2023, including 1225 patients. Inclusion criteria covered all patients older than 16 years presenting to the ED, excluding cardiac arrest cases, pregnancy-related complications, and individuals declared dead on arrival. Data were collected using predesigned proformas. Univariate and multivariate logistic regression analyses identified high-risk chief complaints.</p><p><strong>Results: </strong>Of the 1754 patients screened, 1225 were included in the analysis. Thirty-four complaints were identified, with six deemed high risk. Specific complaints such as shortness of breath (odds ratio [OR] 43.691, 95% confidence interval [CI] 20.033-95.291, <i>P</i> = 0.001), altered mental status (OR: 6.243, 95% CI: 3.282-11.876, <i>P</i> < 0.001), hematemesis (OR: 3.88, 95% CI: 2.019-7.454, <i>P</i> < 0.001), fall from height (OR: 3.875, 95% CI: 1.874-8.014, <i>P</i> < 0.001), weakness of one side (OR: 3.159, 95% CI: 1.656-6.024, <i>P</i> < 0.001), and chest pain (OR: 1.784, 95% CI: 1.22-3.209, <i>P</i> = 0.043) were significantly associated with adverse outcomes (mortality or ICU admission) at 72 h, even after adjusting for age, gender, and comorbidities. Incorporating high-risk complaints into the ATP triage system increased predictive value (OR 3.12 vs. 7.14).</p><p><strong>Conclusion: </strong>Our findings highlight specific chief complaints as valuable indicators for the early identification of patients at risk of 72-h mortality or ICU admission in the ED. Early identification of high-risk patients can enhance early resuscitation, timely referral to higher-level care, and improve patient outcomes.</p>\",\"PeriodicalId\":15692,\"journal\":{\"name\":\"Journal of Emergencies, Trauma, and Shock\",\"volume\":\"18 2\",\"pages\":\"62-68\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12258527/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Emergencies, Trauma, and Shock\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jets.jets_127_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Emergencies, Trauma, and Shock","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jets.jets_127_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
导读:分诊是一个关键的过程,优先考虑患者基于敏锐度,以确保及时护理。病人来到急诊科(ED)是带着抱怨,而不是诊断。根据病史、生命体征、外伤损伤机制和临床表现来确定高危患者。急诊科的主诉可能是独立于其他临床参数的视力。本研究的目的是确定与重症监护病房(ICU)入院或ED出现72小时内死亡率相关的高危主诉。我们还按频率对主诉进行了特征描述,并评估了全印度医学科学研究所分诊方案(ATP)与预测死亡率的高风险主诉的准确性。方法:这项前瞻性观察性研究于2021年3月至2023年10月在新德里AIIMS进行,包括1225名患者。纳入标准包括所有到急诊科就诊的16岁以上患者,不包括心脏骤停病例、妊娠相关并发症和抵达时宣布死亡的患者。使用预先设计的表格收集数据。单因素和多因素logistic回归分析确定了高危主诉。结果:在筛选的1754例患者中,1225例纳入分析。共发现34起投诉,其中6起被视为高风险。具体的主诉如呼吸短促(优势比[OR] 43.691, 95%可信区间[CI] 20.033-95.291, P = 0.001)、精神状态改变(OR: 6.243, 95% CI: 3.283 -11.876, P < 0.001)、吐血(OR: 3.88, 95% CI: 2.019-7.454, P < 0.001)、高空跌落(OR: 3.875, 95% CI: 1.874-8.014, P < 0.001)、单侧无力(OR: 3.159, 95% CI: 1.656-6.024, P < 0.001)、胸痛(OR: 1.784, 95% CI:1.22-3.209, P = 0.043)与72小时不良结局(死亡率或ICU入院率)显著相关,即使在调整了年龄、性别和合并症后也是如此。将高风险投诉纳入ATP分诊系统增加了预测值(OR 3.12 vs. 7.14)。结论:我们的研究结果强调了特定的主诉是早期识别有72小时死亡风险或在急诊科进入ICU的患者的有价值的指标。早期识别高危患者可以加强早期复苏,及时转诊到更高级别的护理,改善患者预后。
Association of Presenting Complaint at Triage with 72-h Mortality and Intensive Care Admission.
Introduction: Triage is a critical process in prioritizing patients based on acuity to ensure timely care. Patients arrive at the emergency department (ED) with complaints, not diagnoses. High-risk patients are identified based on history, vital signs, mechanism of injury in trauma, and clinical findings. Chief complaints in the ED may suggest acuity independent of other clinical parameters. The objective of this study was to identify high-risk chief complaints associated with intensive care unit (ICU) admission or mortality within 72 h of ED presentation. We also characterized the chief complaints by frequency and evaluated the accuracy of the All India Institute of Medical Sciences Triage Protocol (ATP) in conjunction with high-risk complaints for predicting mortality.
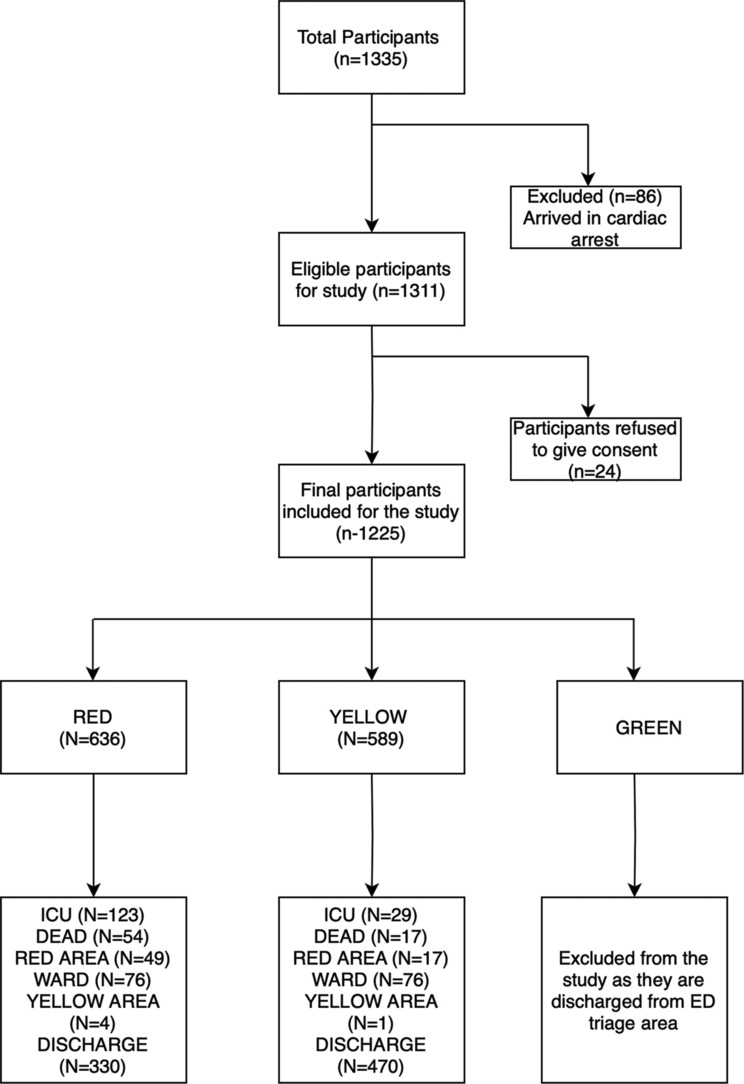
Methods: This prospective observational study was conducted at AIIMS, New Delhi, from March 2021 to October 2023, including 1225 patients. Inclusion criteria covered all patients older than 16 years presenting to the ED, excluding cardiac arrest cases, pregnancy-related complications, and individuals declared dead on arrival. Data were collected using predesigned proformas. Univariate and multivariate logistic regression analyses identified high-risk chief complaints.
Results: Of the 1754 patients screened, 1225 were included in the analysis. Thirty-four complaints were identified, with six deemed high risk. Specific complaints such as shortness of breath (odds ratio [OR] 43.691, 95% confidence interval [CI] 20.033-95.291, P = 0.001), altered mental status (OR: 6.243, 95% CI: 3.282-11.876, P < 0.001), hematemesis (OR: 3.88, 95% CI: 2.019-7.454, P < 0.001), fall from height (OR: 3.875, 95% CI: 1.874-8.014, P < 0.001), weakness of one side (OR: 3.159, 95% CI: 1.656-6.024, P < 0.001), and chest pain (OR: 1.784, 95% CI: 1.22-3.209, P = 0.043) were significantly associated with adverse outcomes (mortality or ICU admission) at 72 h, even after adjusting for age, gender, and comorbidities. Incorporating high-risk complaints into the ATP triage system increased predictive value (OR 3.12 vs. 7.14).
Conclusion: Our findings highlight specific chief complaints as valuable indicators for the early identification of patients at risk of 72-h mortality or ICU admission in the ED. Early identification of high-risk patients can enhance early resuscitation, timely referral to higher-level care, and improve patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


