{"title":"术前肠-肝CT比值:预测绞窄性梗阻切除的有用指标。","authors":"Seiichiro Fujishima, Hironori Tsujimoto, Yoshihisa Yaguchi, Hiroyuki Horiguchi, Keita Kouzu, Yusuke Ishibashi, Yujiro Itazaki, Takafumi Suzuki, Naoyuki Uehata, Risa Kariya, Asuma Ide, Hiroshi Shinmoto, Hideki Ueno","doi":"10.1007/s10140-025-02369-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prompt diagnosis of strangulated bowel obstruction (SBO) is critical because delayed recognition can lead to life-threatening complications. This study assessed whether the intestinal-to-liver CT attenuation value ratio-a comparison of ischemic bowel-wall enhancement to liver enhancement-can predict the need for intestinal resection in SBO patients.</p><p><strong>Materials and methods: </strong>We retrospectively analyzed 52 patients who underwent emergency surgery for suspected SBO from 2014 to 2021. Of these, 35 required intestinal resection due to irreversible ischemia (resection group), while 17 did not (no-resection group). Preoperative clinical and imaging findings were compared between groups.</p><p><strong>Results: </strong>The resection group had a longer time from onset to surgery (p = 0.034) and higher leukocyte counts (p = 0.037). CT values of the poorly enhanced intestinal wall and the intestinal-to-liver attenuation ratio were significantly lower in the resection group (p < 0.0001). Multivariate analysis identified time to surgery (OR 5.08; 95% CI 1.106-23.350; p = 0.037) and CT attenuation ratio (OR 15.50; 95% CI 2.622-91.686; p = 0.0025) as independent predictors of resection. When stratified by the median ratio cutoff (< 0.40 vs. ≥ 0.40), resection rates were 92% and 44%, respectively (p = 0.0001). Additionally, CT attenuation ratio had the diagnostic performance (AUROC 0.886; Youden index 0.736; sensitivity 97.1% and specificity 76.5%.) CONCLUSION: An intestinal-to-liver CT attenuation ratio below 0.40 is a strong predictor of intestinal ischemia requiring resection in SBO patients.</p>","PeriodicalId":11623,"journal":{"name":"Emergency Radiology","volume":" ","pages":"581-589"},"PeriodicalIF":1.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12328548/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preoperative intestine-to-liver CT ratio: useful predictor of resection in strangulated obstruction.\",\"authors\":\"Seiichiro Fujishima, Hironori Tsujimoto, Yoshihisa Yaguchi, Hiroyuki Horiguchi, Keita Kouzu, Yusuke Ishibashi, Yujiro Itazaki, Takafumi Suzuki, Naoyuki Uehata, Risa Kariya, Asuma Ide, Hiroshi Shinmoto, Hideki Ueno\",\"doi\":\"10.1007/s10140-025-02369-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prompt diagnosis of strangulated bowel obstruction (SBO) is critical because delayed recognition can lead to life-threatening complications. This study assessed whether the intestinal-to-liver CT attenuation value ratio-a comparison of ischemic bowel-wall enhancement to liver enhancement-can predict the need for intestinal resection in SBO patients.</p><p><strong>Materials and methods: </strong>We retrospectively analyzed 52 patients who underwent emergency surgery for suspected SBO from 2014 to 2021. Of these, 35 required intestinal resection due to irreversible ischemia (resection group), while 17 did not (no-resection group). Preoperative clinical and imaging findings were compared between groups.</p><p><strong>Results: </strong>The resection group had a longer time from onset to surgery (p = 0.034) and higher leukocyte counts (p = 0.037). CT values of the poorly enhanced intestinal wall and the intestinal-to-liver attenuation ratio were significantly lower in the resection group (p < 0.0001). Multivariate analysis identified time to surgery (OR 5.08; 95% CI 1.106-23.350; p = 0.037) and CT attenuation ratio (OR 15.50; 95% CI 2.622-91.686; p = 0.0025) as independent predictors of resection. When stratified by the median ratio cutoff (< 0.40 vs. ≥ 0.40), resection rates were 92% and 44%, respectively (p = 0.0001). Additionally, CT attenuation ratio had the diagnostic performance (AUROC 0.886; Youden index 0.736; sensitivity 97.1% and specificity 76.5%.) CONCLUSION: An intestinal-to-liver CT attenuation ratio below 0.40 is a strong predictor of intestinal ischemia requiring resection in SBO patients.</p>\",\"PeriodicalId\":11623,\"journal\":{\"name\":\"Emergency Radiology\",\"volume\":\" \",\"pages\":\"581-589\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12328548/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Emergency Radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s10140-025-02369-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10140-025-02369-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Preoperative intestine-to-liver CT ratio: useful predictor of resection in strangulated obstruction.
Background: Prompt diagnosis of strangulated bowel obstruction (SBO) is critical because delayed recognition can lead to life-threatening complications. This study assessed whether the intestinal-to-liver CT attenuation value ratio-a comparison of ischemic bowel-wall enhancement to liver enhancement-can predict the need for intestinal resection in SBO patients.
Materials and methods: We retrospectively analyzed 52 patients who underwent emergency surgery for suspected SBO from 2014 to 2021. Of these, 35 required intestinal resection due to irreversible ischemia (resection group), while 17 did not (no-resection group). Preoperative clinical and imaging findings were compared between groups.
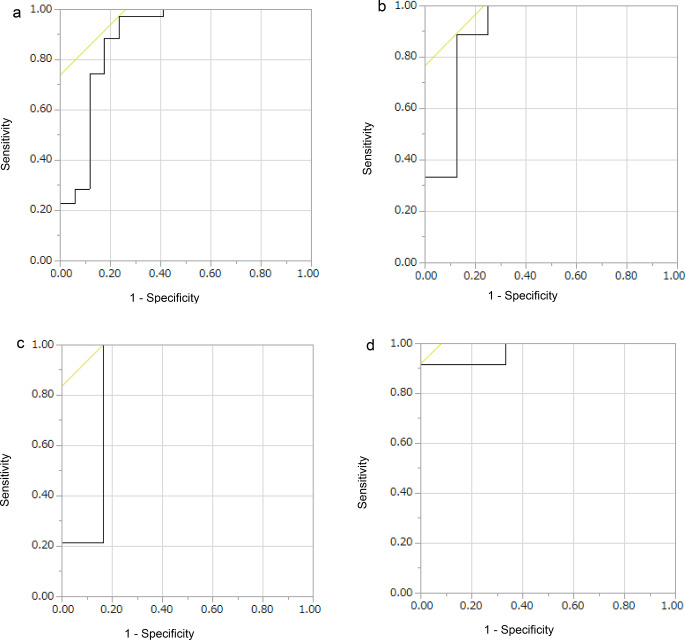
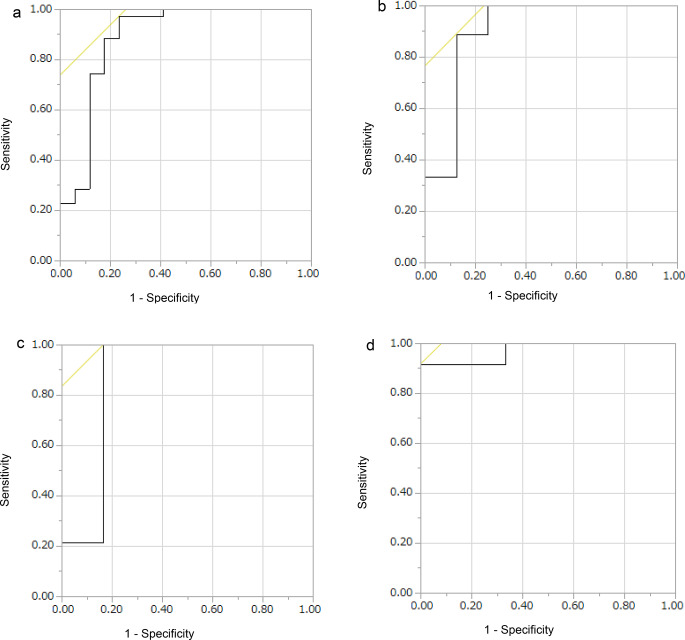
Results: The resection group had a longer time from onset to surgery (p = 0.034) and higher leukocyte counts (p = 0.037). CT values of the poorly enhanced intestinal wall and the intestinal-to-liver attenuation ratio were significantly lower in the resection group (p < 0.0001). Multivariate analysis identified time to surgery (OR 5.08; 95% CI 1.106-23.350; p = 0.037) and CT attenuation ratio (OR 15.50; 95% CI 2.622-91.686; p = 0.0025) as independent predictors of resection. When stratified by the median ratio cutoff (< 0.40 vs. ≥ 0.40), resection rates were 92% and 44%, respectively (p = 0.0001). Additionally, CT attenuation ratio had the diagnostic performance (AUROC 0.886; Youden index 0.736; sensitivity 97.1% and specificity 76.5%.) CONCLUSION: An intestinal-to-liver CT attenuation ratio below 0.40 is a strong predictor of intestinal ischemia requiring resection in SBO patients.
期刊介绍:
To advance and improve the radiologic aspects of emergency careTo establish Emergency Radiology as an area of special interest in the field of diagnostic imagingTo improve methods of education in Emergency RadiologyTo provide, through formal meetings, a mechanism for presentation of scientific papers on various aspects of Emergency Radiology and continuing educationTo promote research in Emergency Radiology by clinical and basic science investigators, including residents and other traineesTo act as the resource body on Emergency Radiology for those interested in emergency patient care Members of the American Society of Emergency Radiology (ASER) receive the Emergency Radiology journal as a benefit of membership!




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


