Hanine O AlMubayedh, Rayd A AlMehizia, Abdul Salam, Razan M AlGhunaim, Othman Mohammed, Abdullah A Alrbiaan, Nada S AlQadheeb
{"title":"感染性休克中氢化可的松停药策略的评价:一项回顾性队列研究。","authors":"Hanine O AlMubayedh, Rayd A AlMehizia, Abdul Salam, Razan M AlGhunaim, Othman Mohammed, Abdullah A Alrbiaan, Nada S AlQadheeb","doi":"10.1097/CCE.0000000000001290","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>While corticosteroid administration in septic shock has been shown to reduce vasopressor requirements and accelerate shock reversal, the optimal discontinuation strategy remains unexplored.</p><p><strong>Objectives: </strong>The purpose of this study was to assess whether rates of hemodynamic instability differ among patients with septic shock undergoing abrupt hydrocortisone discontinuation compared with gradual tapering.</p><p><strong>Design, setting, and participants: </strong>A retrospective cohort study conducted in five medical and surgical ICUs at a tertiary care hospital, involving adult patients (≥ 18 yr) with septic shock who received at least 48 hours of stress-dose hydrocortisone (≥ 200 mg/d).</p><p><strong>Main outcomes and measures: </strong>The primary outcome was hemodynamic instability, defined as vasopressor reinitiation during tapering or within 72 hours of hydrocortisone discontinuation. Secondary outcomes included dysglycemia, duration of mechanical ventilation, ICU and hospital length of stay, and mortality.</p><p><strong>Results: </strong>Patients were grouped based on their hydrocortisone discontinuation strategy into abrupt and gradual tapering groups. A total of 414 patients were included in this evaluation. Gradual tapering was associated with higher rates of hemodynamic instability (29.2% vs. 12.9%; p < 0.001), more frequent dysglycemia (59.4% vs. 43.1%; p < 0.001), longer hydrocortisone use (9.9 vs. 4.1 d; p < 0.001), and extended mechanical ventilation (20 vs. 15 d; p = 0.014) and ICU stay (23 vs. 17 d; p = 0.008). Total hydrocortisone duration was the strongest independent predictor of post-discontinuation hemodynamic instability, regardless of strategy (adjusted odds ratio, 1.083; 95% CI, 1.025-1.145; p = 0.004).</p><p><strong>Conclusions and relevance: </strong>While abrupt hydrocortisone discontinuation was associated with fewer ICU-related adverse events, hydrocortisone duration was the primary factor influencing hemodynamic instability post-discontinuation among patients with septic shock. Prospective studies are needed to determine the optimal discontinuation strategy in septic shock.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 7","pages":"e1290"},"PeriodicalIF":2.7000,"publicationDate":"2025-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12440428/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of Hydrocortisone Discontinuation Strategies in Septic Shock: A Retrospective Cohort Study.\",\"authors\":\"Hanine O AlMubayedh, Rayd A AlMehizia, Abdul Salam, Razan M AlGhunaim, Othman Mohammed, Abdullah A Alrbiaan, Nada S AlQadheeb\",\"doi\":\"10.1097/CCE.0000000000001290\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>While corticosteroid administration in septic shock has been shown to reduce vasopressor requirements and accelerate shock reversal, the optimal discontinuation strategy remains unexplored.</p><p><strong>Objectives: </strong>The purpose of this study was to assess whether rates of hemodynamic instability differ among patients with septic shock undergoing abrupt hydrocortisone discontinuation compared with gradual tapering.</p><p><strong>Design, setting, and participants: </strong>A retrospective cohort study conducted in five medical and surgical ICUs at a tertiary care hospital, involving adult patients (≥ 18 yr) with septic shock who received at least 48 hours of stress-dose hydrocortisone (≥ 200 mg/d).</p><p><strong>Main outcomes and measures: </strong>The primary outcome was hemodynamic instability, defined as vasopressor reinitiation during tapering or within 72 hours of hydrocortisone discontinuation. Secondary outcomes included dysglycemia, duration of mechanical ventilation, ICU and hospital length of stay, and mortality.</p><p><strong>Results: </strong>Patients were grouped based on their hydrocortisone discontinuation strategy into abrupt and gradual tapering groups. A total of 414 patients were included in this evaluation. Gradual tapering was associated with higher rates of hemodynamic instability (29.2% vs. 12.9%; p < 0.001), more frequent dysglycemia (59.4% vs. 43.1%; p < 0.001), longer hydrocortisone use (9.9 vs. 4.1 d; p < 0.001), and extended mechanical ventilation (20 vs. 15 d; p = 0.014) and ICU stay (23 vs. 17 d; p = 0.008). Total hydrocortisone duration was the strongest independent predictor of post-discontinuation hemodynamic instability, regardless of strategy (adjusted odds ratio, 1.083; 95% CI, 1.025-1.145; p = 0.004).</p><p><strong>Conclusions and relevance: </strong>While abrupt hydrocortisone discontinuation was associated with fewer ICU-related adverse events, hydrocortisone duration was the primary factor influencing hemodynamic instability post-discontinuation among patients with septic shock. Prospective studies are needed to determine the optimal discontinuation strategy in septic shock.</p>\",\"PeriodicalId\":93957,\"journal\":{\"name\":\"Critical care explorations\",\"volume\":\"7 7\",\"pages\":\"e1290\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-07-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12440428/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical care explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000001290\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001290","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
重要性:虽然在感染性休克中使用皮质类固醇已被证明可以降低血管加压素的需求并加速休克逆转,但最佳的停药策略仍未被探索。目的:本研究的目的是评估突然停用氢化可的松与逐渐停用氢化可的松相比,感染性休克患者的血流动力学不稳定率是否存在差异。设计、环境和参与者:在一家三级医院的5个内科和外科icu中进行的一项回顾性队列研究,涉及接受至少48小时应激剂量氢化可的松(≥200mg /d)的感染性休克成年患者(≥18岁)。主要结局和指标:主要结局是血流动力学不稳定,定义为在逐渐减量或氢化可的松停药72小时内血管加压素重新启动。次要结局包括血糖异常、机械通气时间、ICU和住院时间以及死亡率。结果:根据氢化可的松停药策略将患者分为突然停药组和逐渐停药组。本次评估共纳入414例患者。逐渐减量与较高的血流动力学不稳定性相关(29.2% vs 12.9%;P < 0.001),更频繁的血糖异常(59.4%比43.1%;P < 0.001),氢化可的松使用时间更长(9.9 vs 4.1 d;P < 0.001),延长机械通气时间(20 vs 15 d;p = 0.014)和ICU住院时间(23天vs. 17天;P = 0.008)。无论采用何种治疗策略,氢化可的松总持续时间都是停药后血流动力学不稳定的最强独立预测因子(校正优势比,1.083;95% ci, 1.025-1.145;P = 0.004)。结论及相关性:虽然突然停用氢化可的松与icu相关不良事件较少相关,但停用氢化可的松的持续时间是影响脓毒性休克患者停药后血流动力学不稳定的主要因素。需要前瞻性研究来确定感染性休克的最佳停药策略。
Evaluation of Hydrocortisone Discontinuation Strategies in Septic Shock: A Retrospective Cohort Study.
Importance: While corticosteroid administration in septic shock has been shown to reduce vasopressor requirements and accelerate shock reversal, the optimal discontinuation strategy remains unexplored.
Objectives: The purpose of this study was to assess whether rates of hemodynamic instability differ among patients with septic shock undergoing abrupt hydrocortisone discontinuation compared with gradual tapering.
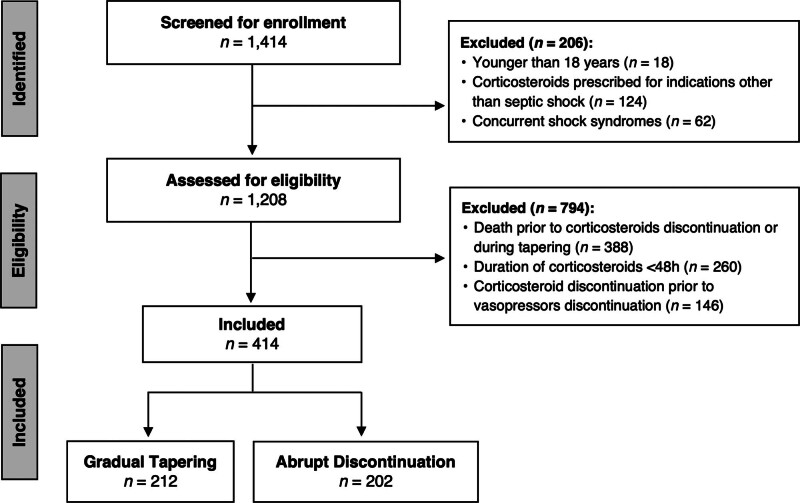
Design, setting, and participants: A retrospective cohort study conducted in five medical and surgical ICUs at a tertiary care hospital, involving adult patients (≥ 18 yr) with septic shock who received at least 48 hours of stress-dose hydrocortisone (≥ 200 mg/d).
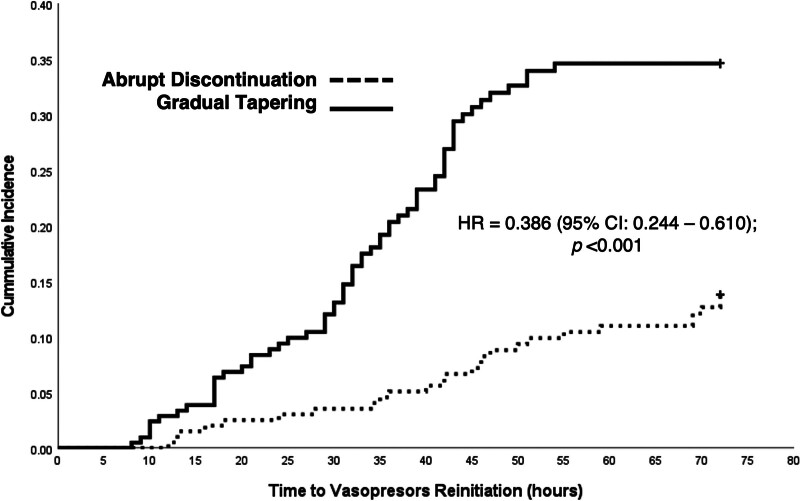
Main outcomes and measures: The primary outcome was hemodynamic instability, defined as vasopressor reinitiation during tapering or within 72 hours of hydrocortisone discontinuation. Secondary outcomes included dysglycemia, duration of mechanical ventilation, ICU and hospital length of stay, and mortality.
Results: Patients were grouped based on their hydrocortisone discontinuation strategy into abrupt and gradual tapering groups. A total of 414 patients were included in this evaluation. Gradual tapering was associated with higher rates of hemodynamic instability (29.2% vs. 12.9%; p < 0.001), more frequent dysglycemia (59.4% vs. 43.1%; p < 0.001), longer hydrocortisone use (9.9 vs. 4.1 d; p < 0.001), and extended mechanical ventilation (20 vs. 15 d; p = 0.014) and ICU stay (23 vs. 17 d; p = 0.008). Total hydrocortisone duration was the strongest independent predictor of post-discontinuation hemodynamic instability, regardless of strategy (adjusted odds ratio, 1.083; 95% CI, 1.025-1.145; p = 0.004).
Conclusions and relevance: While abrupt hydrocortisone discontinuation was associated with fewer ICU-related adverse events, hydrocortisone duration was the primary factor influencing hemodynamic instability post-discontinuation among patients with septic shock. Prospective studies are needed to determine the optimal discontinuation strategy in septic shock.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


