{"title":"一种新的临床评分预测急诊科出现眩晕或头晕的急性缺血性脑卒中的诊断性能。","authors":"Tuğba Sanalp Menekşe, İlker Şirin, Yavuz Otal","doi":"10.1186/s12873-025-01284-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Vertigo or dizziness (VDS) are common reasons for emergency department (ED) visits and pose significant challenges in the early identification of acute ischemic stroke (AIS). The TriAGe + score was developed to predict AIS in patients presenting with VDS without relying on neuroimaging; however, its diagnostic accuracy compared with ABCD-based scores remains uncertain. This study aims to evaluate the efficacy of the TriAGe + score in distinguishing central ischemic causes from peripheral etiologies in patients with VDS and to compare its predictive accuracy for AIS, including posterior circulation infarctions (PCIs), with that of the ABCD2, ABCD3, and ABCD3-I scores.</p><p><strong>Methods: </strong>This retrospective cohort study evaluated 1,138 patients who presented to a tertiary ED with VDS complaints between January 2023 and July 2024. After applying the exclusion criteria, 886 patients were included. All patients underwent diffusion-weighted magnetic resonance imaging within 72 h for diagnostic confirmation. On the basis of the imaging results, 210 patients were diagnosed with AIS, while 676 patients without findings consistent with AIS were considered the control group. The predictive performance of the TriAGe + and ABCD scores was evaluated in both groups via logistic regression and receiver operating characteristic (ROC) analyses.</p><p><strong>Results: </strong>PCIs accounted for 74.3% of all AIS cases. The TriAGe + score demonstrated greater diagnostic accuracy than did the ABCD scores in the ROC analysis among all patients (AUC = 0.979; 95% confidence interval [CI]: 0.967-0.987). For the diagnosis of AIS in all patients, the TriAGe + score had a cutoff value of > 7, with a sensitivity of 91% and a specificity of 91.3%. In patients without focal weakness or sensory loss, the TriAGe + score remained a strong predictor of AIS, with a cutoff value of 5, yielding a sensitivity of 97.5% and a specificity of 80.9% (AUC = 0.950; 95% CI: 0.932-0.964).</p><p><strong>Conclusion: </strong>The TriAGe + score is useful in the diagnosis of AIS in patients presenting to the ED with VDS complaints. It outperforms ABCD scores in sensitivity and specificity, particularly in cases without focal neurological deficits. Implementing the TriAGE + score may optimize neuroimaging use, reduce healthcare costs, and improve ED efficiency by assisting clinicians in prioritizing high-risk patients.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"127"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12261693/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic performance of a novel clinical score for predicting acute ischemic stroke in emergency department patients presenting with vertigo or dizziness.\",\"authors\":\"Tuğba Sanalp Menekşe, İlker Şirin, Yavuz Otal\",\"doi\":\"10.1186/s12873-025-01284-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Vertigo or dizziness (VDS) are common reasons for emergency department (ED) visits and pose significant challenges in the early identification of acute ischemic stroke (AIS). The TriAGe + score was developed to predict AIS in patients presenting with VDS without relying on neuroimaging; however, its diagnostic accuracy compared with ABCD-based scores remains uncertain. This study aims to evaluate the efficacy of the TriAGe + score in distinguishing central ischemic causes from peripheral etiologies in patients with VDS and to compare its predictive accuracy for AIS, including posterior circulation infarctions (PCIs), with that of the ABCD2, ABCD3, and ABCD3-I scores.</p><p><strong>Methods: </strong>This retrospective cohort study evaluated 1,138 patients who presented to a tertiary ED with VDS complaints between January 2023 and July 2024. After applying the exclusion criteria, 886 patients were included. All patients underwent diffusion-weighted magnetic resonance imaging within 72 h for diagnostic confirmation. On the basis of the imaging results, 210 patients were diagnosed with AIS, while 676 patients without findings consistent with AIS were considered the control group. The predictive performance of the TriAGe + and ABCD scores was evaluated in both groups via logistic regression and receiver operating characteristic (ROC) analyses.</p><p><strong>Results: </strong>PCIs accounted for 74.3% of all AIS cases. The TriAGe + score demonstrated greater diagnostic accuracy than did the ABCD scores in the ROC analysis among all patients (AUC = 0.979; 95% confidence interval [CI]: 0.967-0.987). For the diagnosis of AIS in all patients, the TriAGe + score had a cutoff value of > 7, with a sensitivity of 91% and a specificity of 91.3%. In patients without focal weakness or sensory loss, the TriAGe + score remained a strong predictor of AIS, with a cutoff value of 5, yielding a sensitivity of 97.5% and a specificity of 80.9% (AUC = 0.950; 95% CI: 0.932-0.964).</p><p><strong>Conclusion: </strong>The TriAGe + score is useful in the diagnosis of AIS in patients presenting to the ED with VDS complaints. It outperforms ABCD scores in sensitivity and specificity, particularly in cases without focal neurological deficits. Implementing the TriAGE + score may optimize neuroimaging use, reduce healthcare costs, and improve ED efficiency by assisting clinicians in prioritizing high-risk patients.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>\",\"PeriodicalId\":9002,\"journal\":{\"name\":\"BMC Emergency Medicine\",\"volume\":\"25 1\",\"pages\":\"127\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12261693/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Emergency Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12873-025-01284-y\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01284-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Diagnostic performance of a novel clinical score for predicting acute ischemic stroke in emergency department patients presenting with vertigo or dizziness.
Background: Vertigo or dizziness (VDS) are common reasons for emergency department (ED) visits and pose significant challenges in the early identification of acute ischemic stroke (AIS). The TriAGe + score was developed to predict AIS in patients presenting with VDS without relying on neuroimaging; however, its diagnostic accuracy compared with ABCD-based scores remains uncertain. This study aims to evaluate the efficacy of the TriAGe + score in distinguishing central ischemic causes from peripheral etiologies in patients with VDS and to compare its predictive accuracy for AIS, including posterior circulation infarctions (PCIs), with that of the ABCD2, ABCD3, and ABCD3-I scores.
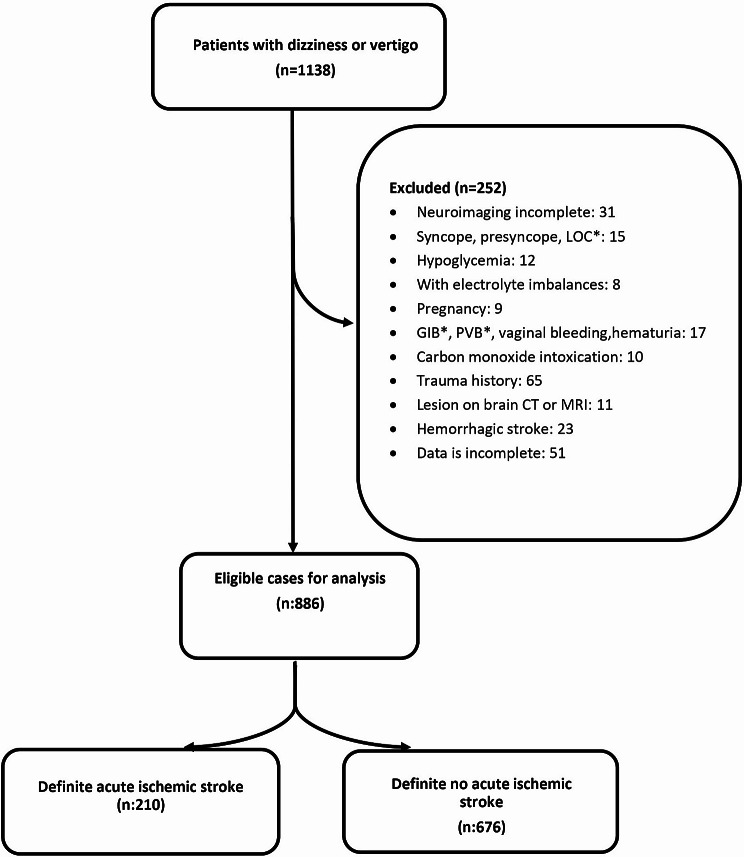
Methods: This retrospective cohort study evaluated 1,138 patients who presented to a tertiary ED with VDS complaints between January 2023 and July 2024. After applying the exclusion criteria, 886 patients were included. All patients underwent diffusion-weighted magnetic resonance imaging within 72 h for diagnostic confirmation. On the basis of the imaging results, 210 patients were diagnosed with AIS, while 676 patients without findings consistent with AIS were considered the control group. The predictive performance of the TriAGe + and ABCD scores was evaluated in both groups via logistic regression and receiver operating characteristic (ROC) analyses.
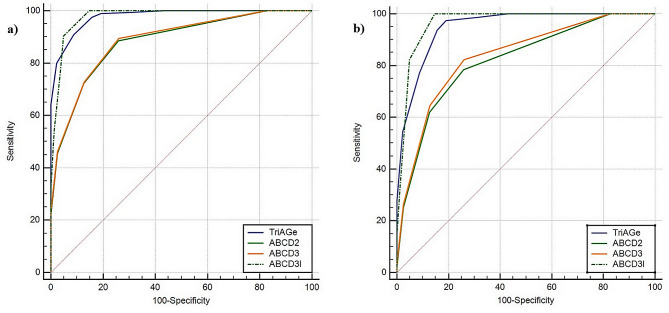
Results: PCIs accounted for 74.3% of all AIS cases. The TriAGe + score demonstrated greater diagnostic accuracy than did the ABCD scores in the ROC analysis among all patients (AUC = 0.979; 95% confidence interval [CI]: 0.967-0.987). For the diagnosis of AIS in all patients, the TriAGe + score had a cutoff value of > 7, with a sensitivity of 91% and a specificity of 91.3%. In patients without focal weakness or sensory loss, the TriAGe + score remained a strong predictor of AIS, with a cutoff value of 5, yielding a sensitivity of 97.5% and a specificity of 80.9% (AUC = 0.950; 95% CI: 0.932-0.964).
Conclusion: The TriAGe + score is useful in the diagnosis of AIS in patients presenting to the ED with VDS complaints. It outperforms ABCD scores in sensitivity and specificity, particularly in cases without focal neurological deficits. Implementing the TriAGE + score may optimize neuroimaging use, reduce healthcare costs, and improve ED efficiency by assisting clinicians in prioritizing high-risk patients.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


