Armando Cuesta Amigo , Nazrin Bakhshaliyeva , Javier García Septiem , Enrique Alday Muñoz
{"title":"门诊大手术中麻醉技术对直肠手术患者出院时间的影响。","authors":"Armando Cuesta Amigo , Nazrin Bakhshaliyeva , Javier García Septiem , Enrique Alday Muñoz","doi":"10.1016/j.cireng.2025.800157","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><div>The present study aims to compare the length of postoperative stay in outpatient surgery (OS) setting of patients undergoing anorectal surgery in four different anaesthetic techniques: local anaesthesia with deep sedation (LA + DS), low-dose spinal anaesthesia (LDSA) (less than 5 mg of hyperbaric bupivacaine or less than 20 mg of hyperbaric prilocaine), high-dose spinal anaesthesia (HDSA), and general anaesthesia (GA). Secondary outcomes include analysing postoperative complications and their relationship with the chosen anaesthetic technique.</div></div><div><h3>Methods</h3><div>Retrospective observational study of patients who underwent scheduled proctological surgery between January 2018 and September 2021. Patients were classified into four groups according to the anaesthetic technique used. The primary outcomes were the length of stay in AS, the need for postoperative opioids, postoperative nausea and vomiting, acute urinary retention, and failure to complete the AS regimen (unscheduled admission to the ward or visit to the emergency room in the first 24 h with or without hospital admission).</div></div><div><h3>Results</h3><div>Out of 337 patients, 137 (40.4%) received HDSA, 68 (20.5%) LDSA, 106 (31.3%) GA, and 26 (7.7%) LA + DS. The longest median stay (226 min) was associated with HDSA (p < 0.001). The shortest time was recorded with LA + DS (121 min). Around 2% required opioids. 71% of them were operated under GA (p = 0.06). AUR occurred in 4% of patients, with no significant differences between groups. The rate of PONV was 74% in the GA group compared to 7–19% in the rest of the groups. A higher OS failure rate (15%) was observed in afternoon shifts compared to 5% in morning shifts.</div></div><div><h3>Conclusions</h3><div>In ambulatory proctological surgery, spinal anaesthesia with doses less than 5 mg of bupivacaine or 20 mg of hyperbaric prilocaine is effective and reduces postoperative stay times. General anaesthesia is associated with a higher incidence of nausea, vomiting, and increased need for postoperative opioids.</div></div>","PeriodicalId":93935,"journal":{"name":"Cirugia espanola","volume":"103 8","pages":"Article 800157"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Impact of anesthetic technique on time to discharge of patients undergoing proctological surgery in major outpatient surgery\",\"authors\":\"Armando Cuesta Amigo , Nazrin Bakhshaliyeva , Javier García Septiem , Enrique Alday Muñoz\",\"doi\":\"10.1016/j.cireng.2025.800157\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Introduction</h3><div>The present study aims to compare the length of postoperative stay in outpatient surgery (OS) setting of patients undergoing anorectal surgery in four different anaesthetic techniques: local anaesthesia with deep sedation (LA + DS), low-dose spinal anaesthesia (LDSA) (less than 5 mg of hyperbaric bupivacaine or less than 20 mg of hyperbaric prilocaine), high-dose spinal anaesthesia (HDSA), and general anaesthesia (GA). Secondary outcomes include analysing postoperative complications and their relationship with the chosen anaesthetic technique.</div></div><div><h3>Methods</h3><div>Retrospective observational study of patients who underwent scheduled proctological surgery between January 2018 and September 2021. Patients were classified into four groups according to the anaesthetic technique used. The primary outcomes were the length of stay in AS, the need for postoperative opioids, postoperative nausea and vomiting, acute urinary retention, and failure to complete the AS regimen (unscheduled admission to the ward or visit to the emergency room in the first 24 h with or without hospital admission).</div></div><div><h3>Results</h3><div>Out of 337 patients, 137 (40.4%) received HDSA, 68 (20.5%) LDSA, 106 (31.3%) GA, and 26 (7.7%) LA + DS. The longest median stay (226 min) was associated with HDSA (p < 0.001). The shortest time was recorded with LA + DS (121 min). Around 2% required opioids. 71% of them were operated under GA (p = 0.06). AUR occurred in 4% of patients, with no significant differences between groups. The rate of PONV was 74% in the GA group compared to 7–19% in the rest of the groups. A higher OS failure rate (15%) was observed in afternoon shifts compared to 5% in morning shifts.</div></div><div><h3>Conclusions</h3><div>In ambulatory proctological surgery, spinal anaesthesia with doses less than 5 mg of bupivacaine or 20 mg of hyperbaric prilocaine is effective and reduces postoperative stay times. General anaesthesia is associated with a higher incidence of nausea, vomiting, and increased need for postoperative opioids.</div></div>\",\"PeriodicalId\":93935,\"journal\":{\"name\":\"Cirugia espanola\",\"volume\":\"103 8\",\"pages\":\"Article 800157\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cirugia espanola\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2173507725001413\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cirugia espanola","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2173507725001413","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Impact of anesthetic technique on time to discharge of patients undergoing proctological surgery in major outpatient surgery
Introduction
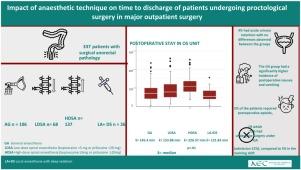
The present study aims to compare the length of postoperative stay in outpatient surgery (OS) setting of patients undergoing anorectal surgery in four different anaesthetic techniques: local anaesthesia with deep sedation (LA + DS), low-dose spinal anaesthesia (LDSA) (less than 5 mg of hyperbaric bupivacaine or less than 20 mg of hyperbaric prilocaine), high-dose spinal anaesthesia (HDSA), and general anaesthesia (GA). Secondary outcomes include analysing postoperative complications and their relationship with the chosen anaesthetic technique.
Methods
Retrospective observational study of patients who underwent scheduled proctological surgery between January 2018 and September 2021. Patients were classified into four groups according to the anaesthetic technique used. The primary outcomes were the length of stay in AS, the need for postoperative opioids, postoperative nausea and vomiting, acute urinary retention, and failure to complete the AS regimen (unscheduled admission to the ward or visit to the emergency room in the first 24 h with or without hospital admission).
Results
Out of 337 patients, 137 (40.4%) received HDSA, 68 (20.5%) LDSA, 106 (31.3%) GA, and 26 (7.7%) LA + DS. The longest median stay (226 min) was associated with HDSA (p < 0.001). The shortest time was recorded with LA + DS (121 min). Around 2% required opioids. 71% of them were operated under GA (p = 0.06). AUR occurred in 4% of patients, with no significant differences between groups. The rate of PONV was 74% in the GA group compared to 7–19% in the rest of the groups. A higher OS failure rate (15%) was observed in afternoon shifts compared to 5% in morning shifts.
Conclusions
In ambulatory proctological surgery, spinal anaesthesia with doses less than 5 mg of bupivacaine or 20 mg of hyperbaric prilocaine is effective and reduces postoperative stay times. General anaesthesia is associated with a higher incidence of nausea, vomiting, and increased need for postoperative opioids.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


