{"title":"预防性苯肾上腺素与去甲肾上腺素对轴向麻醉下剖宫产胎母结局的影响:一项系统综述和荟萃分析。","authors":"Anjishnujit Bandyopadhyay, Chhavi Sawhney, Partha Haldar, Sharmishtha Pathak","doi":"10.4103/ija.ija_1063_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>The prevention of hypotension in parturients scheduled for caesarean section is of utmost importance for improving foeto-maternal outcomes. We compared the prophylactic use of phenylephrine (PE) and norepinephrine (NE) on foeto-maternal outcomes in women undergoing caesarean delivery under neuraxial anaesthesia. Umbilical artery (UA) pH was the primary objective, and umbilical vein (UV) pH, APGAR scores, incidence of bradycardia, hypotension, and hypertension were secondary objectives.</p><p><strong>Methods: </strong>PubMed, EMBASE, Web of Science, Google Scholar, and CENTRAL databases were searched to identify all relevant randomised controlled trials (RCTs) published up to April 2023, further updated till May 2025. Our review was prospectively registered with PROSPERO (ID: CRD42023429328). The effect of PE and NE on UA pH was our primary outcome. The quality of evidence of outcomes was graded using the GRADE methodology. Only RCTs involving term pregnant females undergoing caesarean section under neuraxial anaesthesia were included.</p><p><strong>Results: </strong>Seventeen trials (2138 patients) were included in the final analysis. NE and PE were comparable in terms of UA and UV pH, with standardised mean difference (SMD) of 0.18 [95% confidence interval (CI): -0.09; 0.45] (I<sup>2</sup> = 81%, <i>P</i> < 0.01) and -0.39 (95% CI: -0.82; 0.04) (I<sup>2</sup> = 91%, <i>P</i> < 0.01), respectively. NE group had significantly lesser episodes of bradycardia [Relative Risk (RR): 0.44 (95% CI: 0.34; 0.56) (I<sup>2</sup> = 28%, <i>P</i> = 0.15)] and hypertension [RR: 0.54 (95% CI: 0.33; 0.90) (I<sup>2</sup> = 0%, <i>P</i> = 0.62)], but incidence of hypotension was comparable between groups [RR: 0.99 (95% CI: 0.82; 1.18) (I<sup>2</sup> = 18%, <i>P</i> = 0.25)]. Trial sequential analysis revealed that the required information size was reached for the outcome of bradycardia only.</p><p><strong>Conclusion: </strong>There is insufficient evidence to recommend using NE preemptively to improve foetal outcomes. Further studies are recommended to validate its effect.</p>","PeriodicalId":13339,"journal":{"name":"Indian Journal of Anaesthesia","volume":"69 7","pages":"638-649"},"PeriodicalIF":1.9000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12244457/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of prophylactic phenylephrine versus norepinephrine on foeto-maternal outcomes in caesarean delivery under neuraxial anaesthesia: A systematic review and meta-analysis with trial sequential analysis.\",\"authors\":\"Anjishnujit Bandyopadhyay, Chhavi Sawhney, Partha Haldar, Sharmishtha Pathak\",\"doi\":\"10.4103/ija.ija_1063_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and aims: </strong>The prevention of hypotension in parturients scheduled for caesarean section is of utmost importance for improving foeto-maternal outcomes. We compared the prophylactic use of phenylephrine (PE) and norepinephrine (NE) on foeto-maternal outcomes in women undergoing caesarean delivery under neuraxial anaesthesia. Umbilical artery (UA) pH was the primary objective, and umbilical vein (UV) pH, APGAR scores, incidence of bradycardia, hypotension, and hypertension were secondary objectives.</p><p><strong>Methods: </strong>PubMed, EMBASE, Web of Science, Google Scholar, and CENTRAL databases were searched to identify all relevant randomised controlled trials (RCTs) published up to April 2023, further updated till May 2025. Our review was prospectively registered with PROSPERO (ID: CRD42023429328). The effect of PE and NE on UA pH was our primary outcome. The quality of evidence of outcomes was graded using the GRADE methodology. Only RCTs involving term pregnant females undergoing caesarean section under neuraxial anaesthesia were included.</p><p><strong>Results: </strong>Seventeen trials (2138 patients) were included in the final analysis. NE and PE were comparable in terms of UA and UV pH, with standardised mean difference (SMD) of 0.18 [95% confidence interval (CI): -0.09; 0.45] (I<sup>2</sup> = 81%, <i>P</i> < 0.01) and -0.39 (95% CI: -0.82; 0.04) (I<sup>2</sup> = 91%, <i>P</i> < 0.01), respectively. NE group had significantly lesser episodes of bradycardia [Relative Risk (RR): 0.44 (95% CI: 0.34; 0.56) (I<sup>2</sup> = 28%, <i>P</i> = 0.15)] and hypertension [RR: 0.54 (95% CI: 0.33; 0.90) (I<sup>2</sup> = 0%, <i>P</i> = 0.62)], but incidence of hypotension was comparable between groups [RR: 0.99 (95% CI: 0.82; 1.18) (I<sup>2</sup> = 18%, <i>P</i> = 0.25)]. Trial sequential analysis revealed that the required information size was reached for the outcome of bradycardia only.</p><p><strong>Conclusion: </strong>There is insufficient evidence to recommend using NE preemptively to improve foetal outcomes. Further studies are recommended to validate its effect.</p>\",\"PeriodicalId\":13339,\"journal\":{\"name\":\"Indian Journal of Anaesthesia\",\"volume\":\"69 7\",\"pages\":\"638-649\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12244457/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Indian Journal of Anaesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/ija.ija_1063_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ija.ija_1063_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:预防剖宫产患者低血压对改善胎母结局至关重要。我们比较了预防性使用苯肾上腺素(PE)和去甲肾上腺素(NE)对接受轴向麻醉的剖宫产妇女的胎母结局的影响。脐动脉(UA) pH值是主要目标,脐静脉(UV) pH值、APGAR评分、心动过缓、低血压和高血压的发生率是次要目标。方法:检索PubMed、EMBASE、Web of Science、b谷歌Scholar和CENTRAL数据库,确定截至2023年4月(进一步更新至2025年5月)发表的所有相关随机对照试验(rct)。我们的研究在PROSPERO进行了前瞻性注册(ID: CRD42023429328)。PE和NE对UA pH的影响是我们的主要结局。使用GRADE方法对结果的证据质量进行分级。仅纳入了在轴向麻醉下进行剖宫产的足月孕妇的随机对照试验。结果:17项试验(2138例)纳入最终分析。NE和PE在UA和UV pH方面具有可比性,标准化平均差(SMD)为0.18[95%置信区间(CI): -0.09;0.45) (I2 = 81%, P < 0.01)和-0.39(95%可信区间:-0.82;0.04) (I2 = 91%, P < 0.01)。NE组的心动过缓发作明显减少[相对危险度(RR): 0.44 (95% CI: 0.34;0.56) (I2 = 28%, P = 0.15)]和高血压[RR: 0.54 (95% CI: 0.33;0.90) (I2 = 0%, P = 0.62)],但两组间低血压发生率相当[RR: 0.99 (95% CI: 0.82;1.18) (i2 = 18%, p = 0.25)]。试验序列分析显示,只有心动过缓的结果达到了所需的信息量。结论:没有足够的证据建议使用NE预先改善胎儿结局。建议进一步研究以验证其效果。
Effect of prophylactic phenylephrine versus norepinephrine on foeto-maternal outcomes in caesarean delivery under neuraxial anaesthesia: A systematic review and meta-analysis with trial sequential analysis.
Background and aims: The prevention of hypotension in parturients scheduled for caesarean section is of utmost importance for improving foeto-maternal outcomes. We compared the prophylactic use of phenylephrine (PE) and norepinephrine (NE) on foeto-maternal outcomes in women undergoing caesarean delivery under neuraxial anaesthesia. Umbilical artery (UA) pH was the primary objective, and umbilical vein (UV) pH, APGAR scores, incidence of bradycardia, hypotension, and hypertension were secondary objectives.
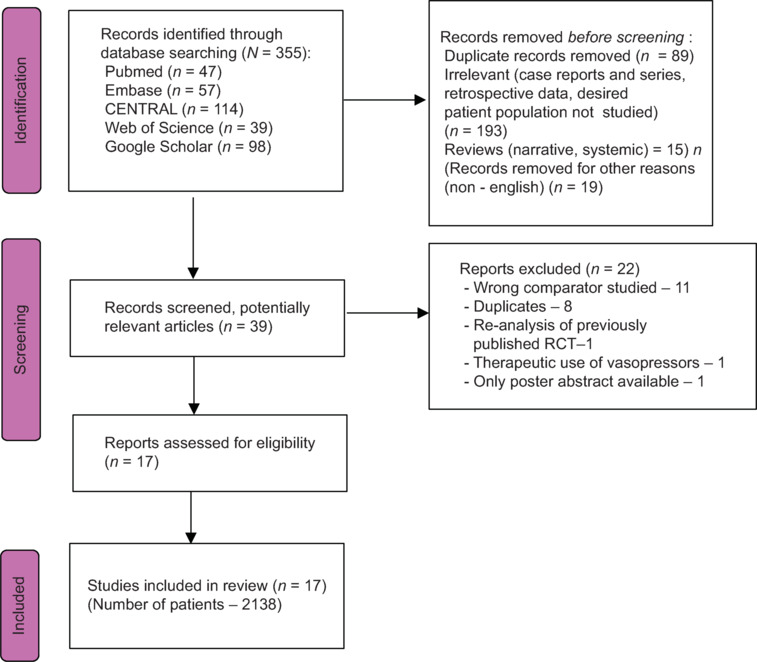
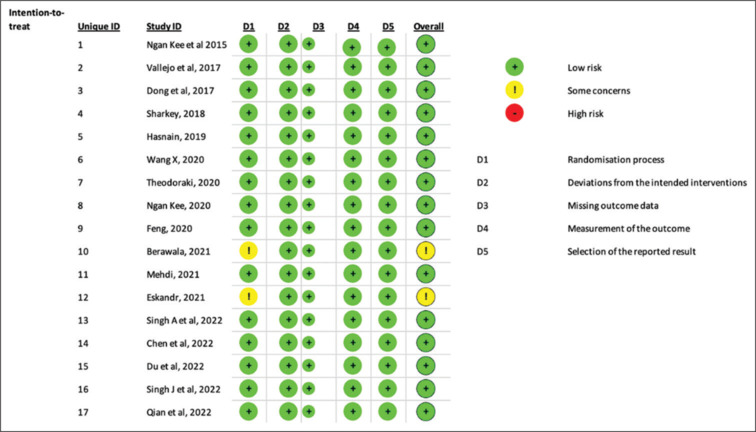
Methods: PubMed, EMBASE, Web of Science, Google Scholar, and CENTRAL databases were searched to identify all relevant randomised controlled trials (RCTs) published up to April 2023, further updated till May 2025. Our review was prospectively registered with PROSPERO (ID: CRD42023429328). The effect of PE and NE on UA pH was our primary outcome. The quality of evidence of outcomes was graded using the GRADE methodology. Only RCTs involving term pregnant females undergoing caesarean section under neuraxial anaesthesia were included.
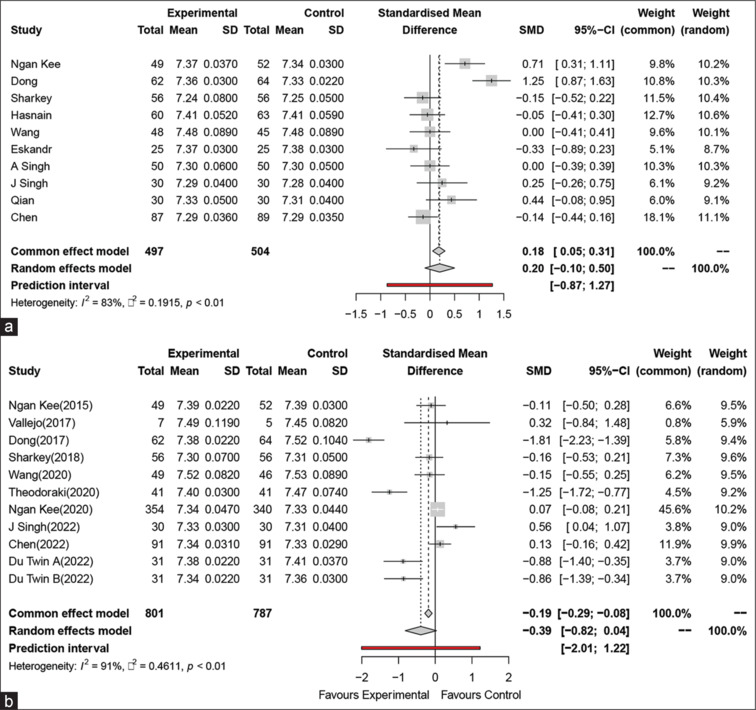
Results: Seventeen trials (2138 patients) were included in the final analysis. NE and PE were comparable in terms of UA and UV pH, with standardised mean difference (SMD) of 0.18 [95% confidence interval (CI): -0.09; 0.45] (I2 = 81%, P < 0.01) and -0.39 (95% CI: -0.82; 0.04) (I2 = 91%, P < 0.01), respectively. NE group had significantly lesser episodes of bradycardia [Relative Risk (RR): 0.44 (95% CI: 0.34; 0.56) (I2 = 28%, P = 0.15)] and hypertension [RR: 0.54 (95% CI: 0.33; 0.90) (I2 = 0%, P = 0.62)], but incidence of hypotension was comparable between groups [RR: 0.99 (95% CI: 0.82; 1.18) (I2 = 18%, P = 0.25)]. Trial sequential analysis revealed that the required information size was reached for the outcome of bradycardia only.
Conclusion: There is insufficient evidence to recommend using NE preemptively to improve foetal outcomes. Further studies are recommended to validate its effect.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


