Letian Huang, Shuling Zhang, Li Sun, Jietao Ma, Chengbo Han
{"title":"表皮生长因子受体-酪氨酸激酶抑制剂耐药Chemotherapy-Naïve晚期非小细胞肺癌:基于8项随机试验的荟萃分析","authors":"Letian Huang, Shuling Zhang, Li Sun, Jietao Ma, Chengbo Han","doi":"10.1200/PO-24-00907","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The efficacy and safety of combination strategies involving immune checkpoint inhibitors (ICIs) in patients with advanced epidermal growth factor receptor (<i>EGFR</i>)-mutant non-small cell lung cancer (NSCLC) who have developed resistance to EGFR-tyrosine kinase inhibitors (TKIs) remains uncertain.</p><p><strong>Methods: </strong>We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing ICIs combined with chemotherapy with or without antiangiogenic therapy (C/A) versus C/A alone in the treatment of advanced NSCLC after resistance to EGFR-TKIs. We searched databases, including PubMed, Cochrane Library, Embase, Web of Science, and meeting abstracts. Hazard ratios (HRs) and 95% CI for median overall survival (OS) and median progression-free survival (PFS) were calculated. Risk ratios (RRs) and 95% CI were used as indicators of objective response rate (ORR) and adverse events (AEs).</p><p><strong>Results: </strong>Eight RCTs involving 10 cohorts and 2,269 patients were included. Adding ICIs to C/A significantly improved PFS (HR, 0.67 [95% CI, 0.57 to 0.80]; <i>P</i> < .001), OS (HR, 0.89 [95% CI, 0.79 to 0.99]; <i>P</i> = .031), and ORR (RR, 0.80 [95% CI, 0.74 to 0.88]; <i>P</i> < .001) comparedwith C/A alone. Subgroup analyses showed that the benefits were more pronounced in patients with PD-L1 expression ≥50%, specific <i>EGFR</i> mutations (Leu858Arg), absence of Thr790Met mutation, and treatment with pemetrexed-platinum. No significant increase in grade 3 or higher AEs was observed, but rates of discontinuation and specific AEs (rash, hypothyroidism, and hypertension) were significantly higher in the ICI+C/A group.</p><p><strong>Conclusion: </strong>This meta-analysis suggests that the addition of ICIs to C/A may improve survival outcomes in patients with advanced NSCLC after resistance to EGFR-TKIs, particularly in selected subpopulations such as those with high PD-L1 expression or specific <i>EGFR</i> mutations. However, careful monitoring for specific AEs is warranted.</p>","PeriodicalId":14797,"journal":{"name":"JCO precision oncology","volume":"9 ","pages":"e2400907"},"PeriodicalIF":5.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12262128/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immune Checkpoint Inhibitors in Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor-Resistant Chemotherapy-Naïve Advanced Non-Small Cell Lung Cancer: A Meta-Analysis Based on Eight Randomized Trials.\",\"authors\":\"Letian Huang, Shuling Zhang, Li Sun, Jietao Ma, Chengbo Han\",\"doi\":\"10.1200/PO-24-00907\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The efficacy and safety of combination strategies involving immune checkpoint inhibitors (ICIs) in patients with advanced epidermal growth factor receptor (<i>EGFR</i>)-mutant non-small cell lung cancer (NSCLC) who have developed resistance to EGFR-tyrosine kinase inhibitors (TKIs) remains uncertain.</p><p><strong>Methods: </strong>We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing ICIs combined with chemotherapy with or without antiangiogenic therapy (C/A) versus C/A alone in the treatment of advanced NSCLC after resistance to EGFR-TKIs. We searched databases, including PubMed, Cochrane Library, Embase, Web of Science, and meeting abstracts. Hazard ratios (HRs) and 95% CI for median overall survival (OS) and median progression-free survival (PFS) were calculated. Risk ratios (RRs) and 95% CI were used as indicators of objective response rate (ORR) and adverse events (AEs).</p><p><strong>Results: </strong>Eight RCTs involving 10 cohorts and 2,269 patients were included. Adding ICIs to C/A significantly improved PFS (HR, 0.67 [95% CI, 0.57 to 0.80]; <i>P</i> < .001), OS (HR, 0.89 [95% CI, 0.79 to 0.99]; <i>P</i> = .031), and ORR (RR, 0.80 [95% CI, 0.74 to 0.88]; <i>P</i> < .001) comparedwith C/A alone. Subgroup analyses showed that the benefits were more pronounced in patients with PD-L1 expression ≥50%, specific <i>EGFR</i> mutations (Leu858Arg), absence of Thr790Met mutation, and treatment with pemetrexed-platinum. No significant increase in grade 3 or higher AEs was observed, but rates of discontinuation and specific AEs (rash, hypothyroidism, and hypertension) were significantly higher in the ICI+C/A group.</p><p><strong>Conclusion: </strong>This meta-analysis suggests that the addition of ICIs to C/A may improve survival outcomes in patients with advanced NSCLC after resistance to EGFR-TKIs, particularly in selected subpopulations such as those with high PD-L1 expression or specific <i>EGFR</i> mutations. However, careful monitoring for specific AEs is warranted.</p>\",\"PeriodicalId\":14797,\"journal\":{\"name\":\"JCO precision oncology\",\"volume\":\"9 \",\"pages\":\"e2400907\"},\"PeriodicalIF\":5.6000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12262128/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JCO precision oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1200/PO-24-00907\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCO precision oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1200/PO-24-00907","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/10 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Immune Checkpoint Inhibitors in Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitor-Resistant Chemotherapy-Naïve Advanced Non-Small Cell Lung Cancer: A Meta-Analysis Based on Eight Randomized Trials.
Purpose: The efficacy and safety of combination strategies involving immune checkpoint inhibitors (ICIs) in patients with advanced epidermal growth factor receptor (EGFR)-mutant non-small cell lung cancer (NSCLC) who have developed resistance to EGFR-tyrosine kinase inhibitors (TKIs) remains uncertain.
Methods: We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing ICIs combined with chemotherapy with or without antiangiogenic therapy (C/A) versus C/A alone in the treatment of advanced NSCLC after resistance to EGFR-TKIs. We searched databases, including PubMed, Cochrane Library, Embase, Web of Science, and meeting abstracts. Hazard ratios (HRs) and 95% CI for median overall survival (OS) and median progression-free survival (PFS) were calculated. Risk ratios (RRs) and 95% CI were used as indicators of objective response rate (ORR) and adverse events (AEs).
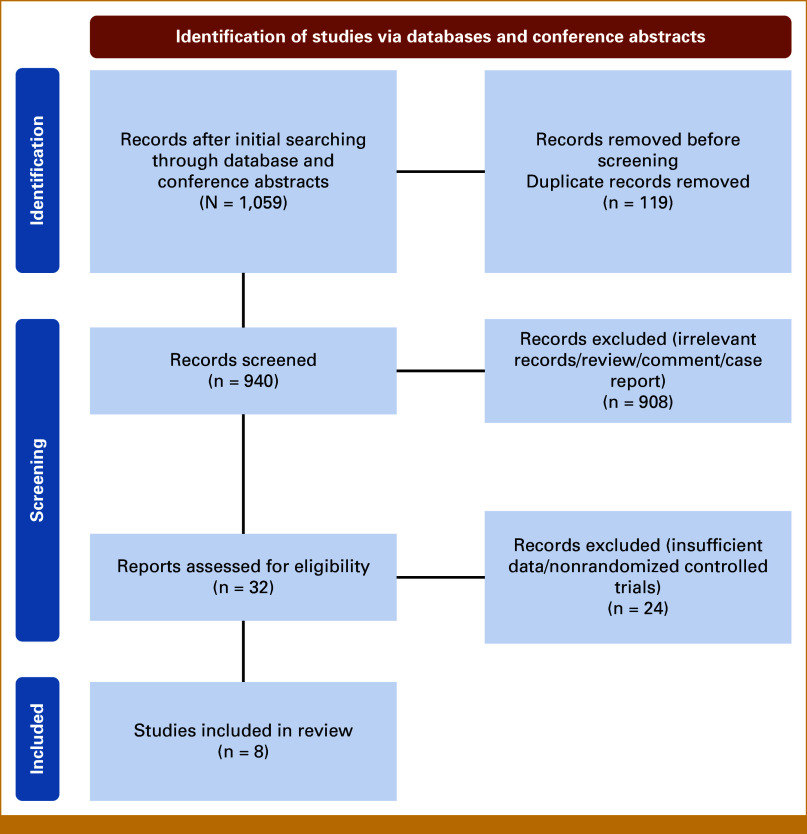
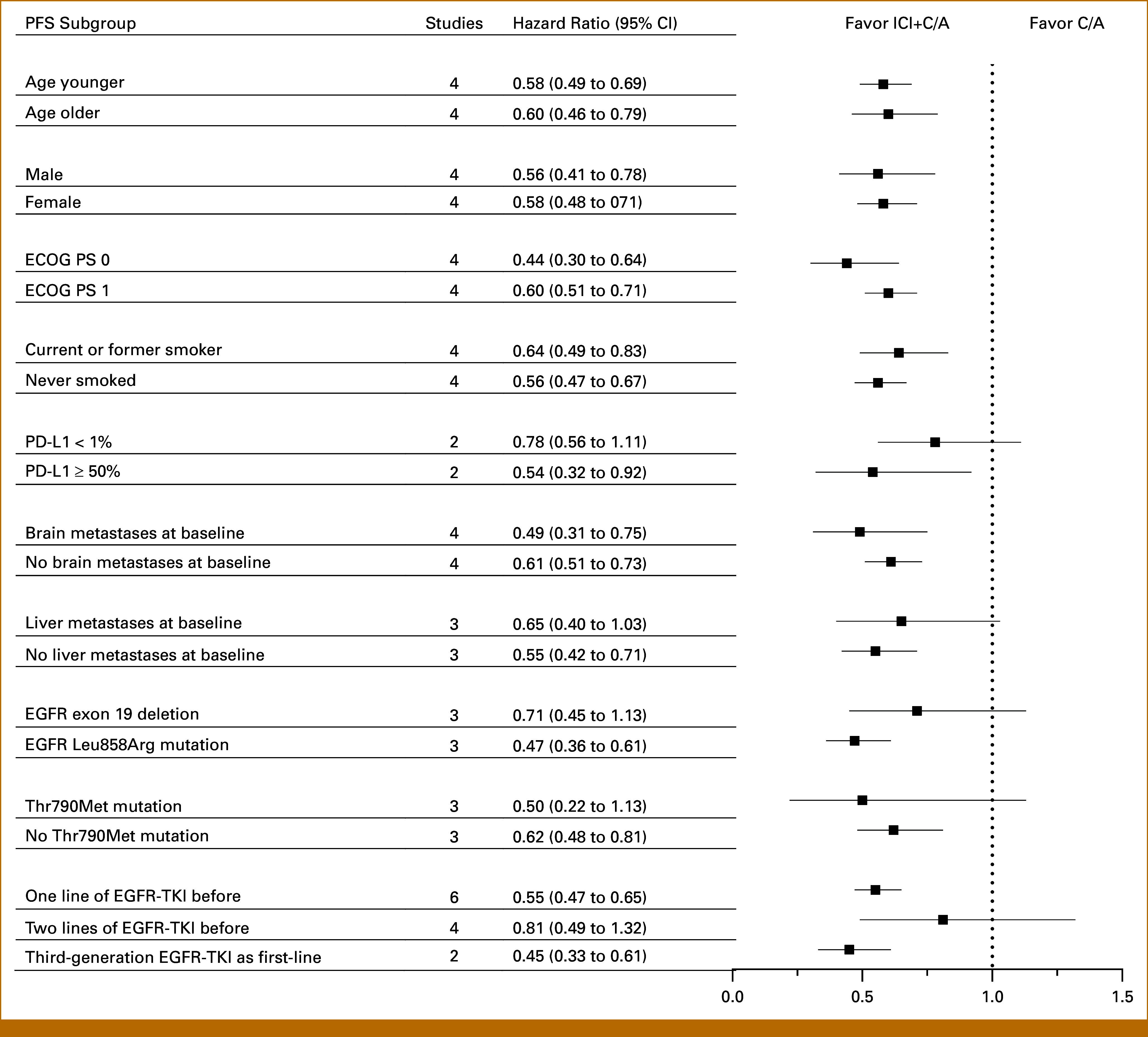
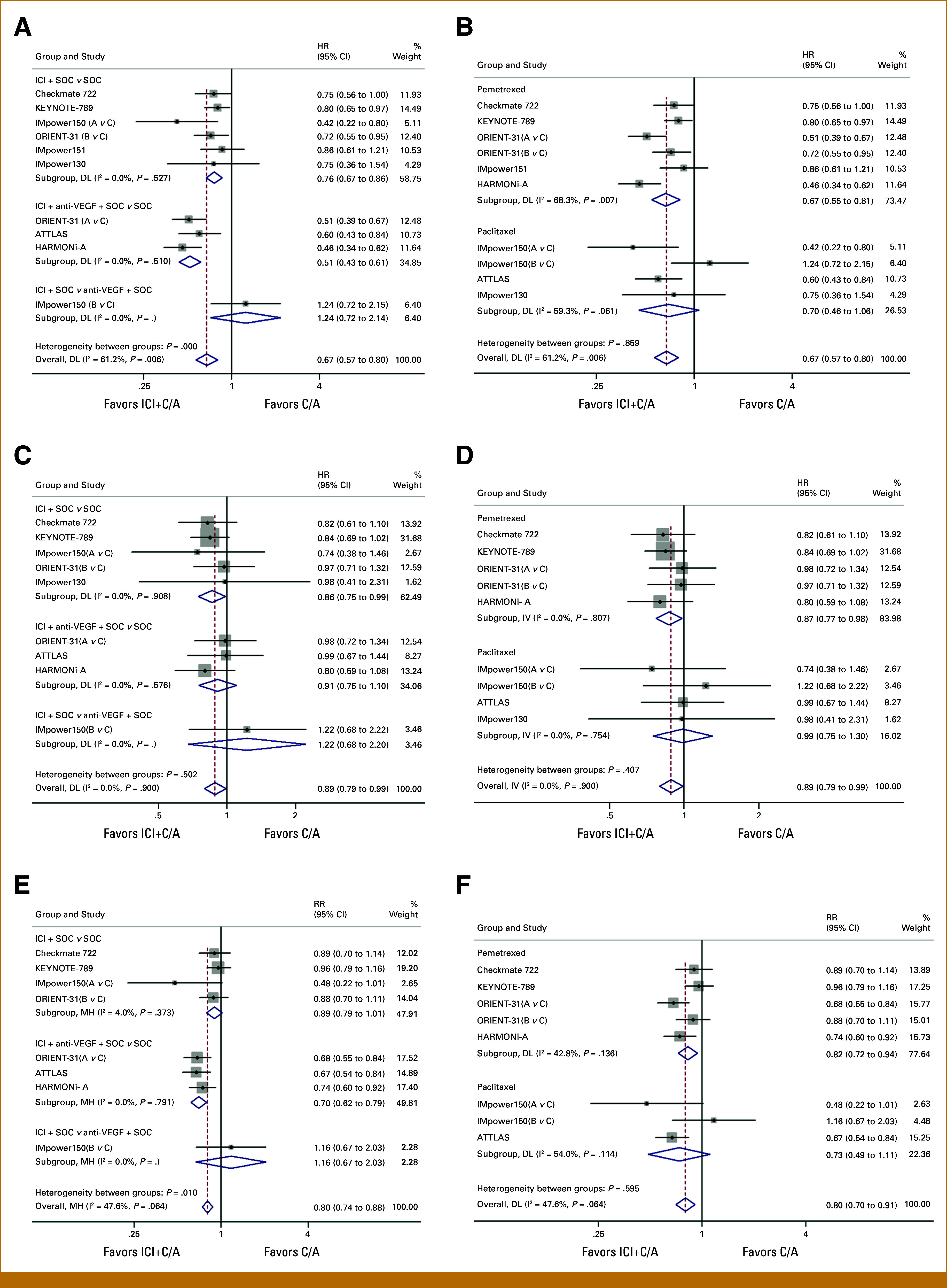
Results: Eight RCTs involving 10 cohorts and 2,269 patients were included. Adding ICIs to C/A significantly improved PFS (HR, 0.67 [95% CI, 0.57 to 0.80]; P < .001), OS (HR, 0.89 [95% CI, 0.79 to 0.99]; P = .031), and ORR (RR, 0.80 [95% CI, 0.74 to 0.88]; P < .001) comparedwith C/A alone. Subgroup analyses showed that the benefits were more pronounced in patients with PD-L1 expression ≥50%, specific EGFR mutations (Leu858Arg), absence of Thr790Met mutation, and treatment with pemetrexed-platinum. No significant increase in grade 3 or higher AEs was observed, but rates of discontinuation and specific AEs (rash, hypothyroidism, and hypertension) were significantly higher in the ICI+C/A group.
Conclusion: This meta-analysis suggests that the addition of ICIs to C/A may improve survival outcomes in patients with advanced NSCLC after resistance to EGFR-TKIs, particularly in selected subpopulations such as those with high PD-L1 expression or specific EGFR mutations. However, careful monitoring for specific AEs is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


