{"title":"晚期、低pd - l1表达的非小细胞肺癌患者的化疗免疫治疗结果和预后因素","authors":"Tae Hata, Tadaaki Yamada, Yasuhiro Goto, Akihiko Amano, Yoshiki Negi, Satoshi Watanabe, Naoki Furuya, Tomohiro Oba, Tatsuki Ikoma, Akira Nakao, Keiko Tanimura, Hirokazu Taniguchi, Akihiro Yoshimura, Tomoya Fukui, Daiki Murata, Kyoichi Kaira, Shinsuke Shiotsu, Makoto Hibino, Asuka Okada, Yusuke Chihara, Hayato Kawachi, Takashi Kijima, Koichi Takayama","doi":"10.1158/2767-9764.CRC-25-0157","DOIUrl":null,"url":null,"abstract":"<p><p>Chemoimmunotherapy is recommended for patients with non-small cell lung cancer (NSCLC) with low PD-L1 expression, but the effect of additional immunotherapy is heterogeneous in this population. To identify patients who do not benefit from the addition of immune checkpoint inhibitors (ICI) to chemotherapy, we conducted a retrospective study at 19 institutions in Japan. We analyzed 851 patients with advanced NSCLC with a PD-L1 tumor proportion score of 1% to 49% who received chemoimmunotherapy (n = 504) or chemotherapy (n = 347) between March 2017 and June 2022. After adjustment by propensity score matching, the median overall survival (OS) was 22.3 months in the chemoimmunotherapy group and 17.0 months in the chemotherapy-alone group (P = 0.01). Multivariate analysis showed that among 12 clinical factors, liver metastases (P = 0.001) and history of antibiotic use (P = 0.02) were independently associated with shorter OS in the chemoimmunotherapy group. Patients with liver metastases (OS, P = 0.4; progression-free survival, P = 0.06) or history of antimicrobial use (OS, P = 0.24; progression-free survival, P = 0.09) did not benefit from the addition of ICI to chemotherapy. Patients with a history of antimicrobial use experienced more severe pneumonitis with chemoimmunotherapy than all patients (P = 0.04). This cohort study showed that liver metastases and prior antimicrobial therapy are the most important clinical factors that attenuate the efficacy of chemoimmunotherapy in patients with low PD-L1 expression.</p><p><strong>Significance: </strong>This study shows that liver metastases and prior antibiotic use are key factors for chemoimmunotherapy in advanced NSCLC cases with low PD-L1 expression. They reduce the benefit of adding ICIs to chemotherapy, underscoring the need for new strategies to improve ICI efficacy in patients.</p>","PeriodicalId":72516,"journal":{"name":"Cancer research communications","volume":" ","pages":"1203-1214"},"PeriodicalIF":3.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12284348/pdf/","citationCount":"0","resultStr":"{\"title\":\"Chemoimmunotherapy Outcomes and Prognostic Factors in Patients with Advanced, Low PD-L1-Expressing Non-Small Cell Lung Cancer.\",\"authors\":\"Tae Hata, Tadaaki Yamada, Yasuhiro Goto, Akihiko Amano, Yoshiki Negi, Satoshi Watanabe, Naoki Furuya, Tomohiro Oba, Tatsuki Ikoma, Akira Nakao, Keiko Tanimura, Hirokazu Taniguchi, Akihiro Yoshimura, Tomoya Fukui, Daiki Murata, Kyoichi Kaira, Shinsuke Shiotsu, Makoto Hibino, Asuka Okada, Yusuke Chihara, Hayato Kawachi, Takashi Kijima, Koichi Takayama\",\"doi\":\"10.1158/2767-9764.CRC-25-0157\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Chemoimmunotherapy is recommended for patients with non-small cell lung cancer (NSCLC) with low PD-L1 expression, but the effect of additional immunotherapy is heterogeneous in this population. To identify patients who do not benefit from the addition of immune checkpoint inhibitors (ICI) to chemotherapy, we conducted a retrospective study at 19 institutions in Japan. We analyzed 851 patients with advanced NSCLC with a PD-L1 tumor proportion score of 1% to 49% who received chemoimmunotherapy (n = 504) or chemotherapy (n = 347) between March 2017 and June 2022. After adjustment by propensity score matching, the median overall survival (OS) was 22.3 months in the chemoimmunotherapy group and 17.0 months in the chemotherapy-alone group (P = 0.01). Multivariate analysis showed that among 12 clinical factors, liver metastases (P = 0.001) and history of antibiotic use (P = 0.02) were independently associated with shorter OS in the chemoimmunotherapy group. Patients with liver metastases (OS, P = 0.4; progression-free survival, P = 0.06) or history of antimicrobial use (OS, P = 0.24; progression-free survival, P = 0.09) did not benefit from the addition of ICI to chemotherapy. Patients with a history of antimicrobial use experienced more severe pneumonitis with chemoimmunotherapy than all patients (P = 0.04). This cohort study showed that liver metastases and prior antimicrobial therapy are the most important clinical factors that attenuate the efficacy of chemoimmunotherapy in patients with low PD-L1 expression.</p><p><strong>Significance: </strong>This study shows that liver metastases and prior antibiotic use are key factors for chemoimmunotherapy in advanced NSCLC cases with low PD-L1 expression. They reduce the benefit of adding ICIs to chemotherapy, underscoring the need for new strategies to improve ICI efficacy in patients.</p>\",\"PeriodicalId\":72516,\"journal\":{\"name\":\"Cancer research communications\",\"volume\":\" \",\"pages\":\"1203-1214\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12284348/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer research communications\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1158/2767-9764.CRC-25-0157\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer research communications","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1158/2767-9764.CRC-25-0157","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
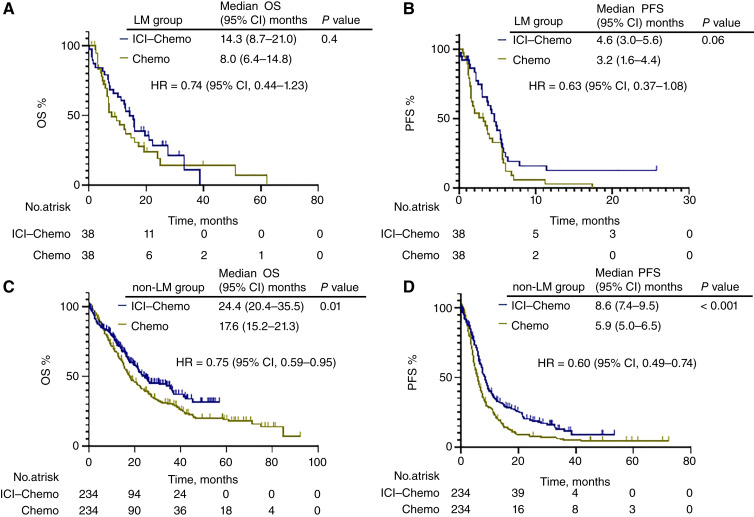
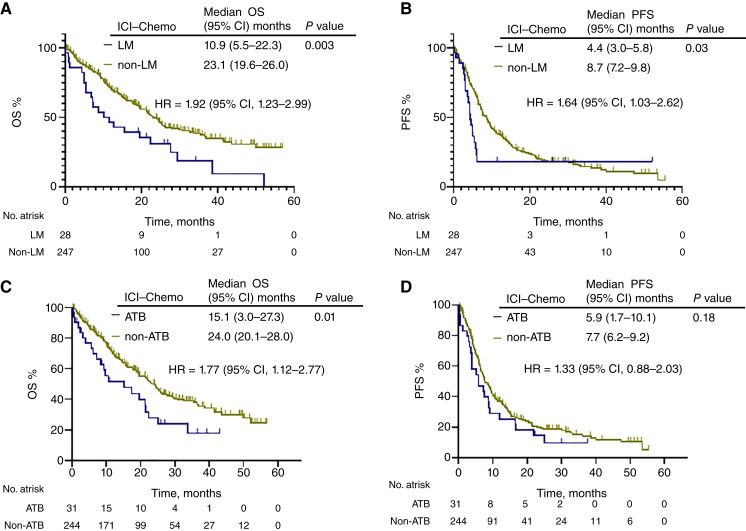
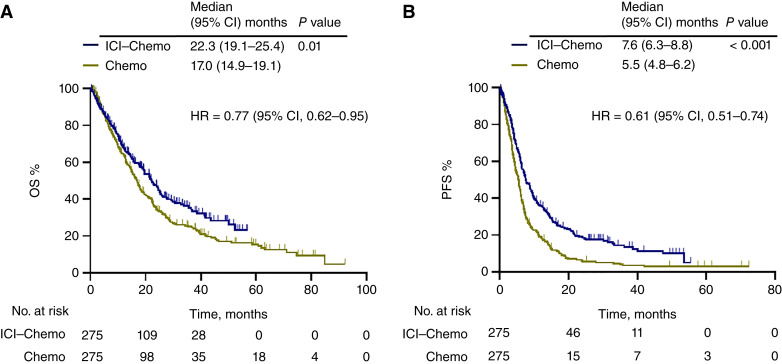
化疗免疫治疗被推荐用于低程序性细胞死亡配体1 (PD-L1)表达的非小细胞肺癌(NSCLC)患者,但在这一人群中,额外免疫治疗的效果是不均匀的。为了确定在化疗中添加免疫检查点抑制剂(ICIs)不能获益的患者,我们在日本的19家机构进行了一项回顾性研究。我们分析了851例晚期NSCLC患者,PD-L1肿瘤比例评分(TPS)为1-49%,在2017年3月至2022年6月期间接受了化疗免疫治疗(n = 504)或化疗(n = 347)。经倾向评分匹配调整后,化疗免疫组的中位总生存期(OS)为22.3个月,单独化疗组的中位总生存期(OS)为17.0个月(P = 0.01)。多因素分析显示,在12个临床因素中,肝转移(P = 0.001)和抗生素使用史(P = 0.02)与化疗免疫治疗组较短的生存期独立相关。肝转移患者(OS, P = 0.4;PFS, P = 0.06)或抗菌药物使用史(OS, P = 0.24;PFS (P = 0.09)并没有从ICI加入化疗中获益。有抗菌药物使用史的患者化疗免疫治疗后肺炎的严重程度高于所有患者(P = 0.04)。本队列研究显示,肝转移或既往抗微生物治疗是降低PD-L1低表达患者化疗免疫治疗疗效的最重要临床因素。
Chemoimmunotherapy Outcomes and Prognostic Factors in Patients with Advanced, Low PD-L1-Expressing Non-Small Cell Lung Cancer.
Chemoimmunotherapy is recommended for patients with non-small cell lung cancer (NSCLC) with low PD-L1 expression, but the effect of additional immunotherapy is heterogeneous in this population. To identify patients who do not benefit from the addition of immune checkpoint inhibitors (ICI) to chemotherapy, we conducted a retrospective study at 19 institutions in Japan. We analyzed 851 patients with advanced NSCLC with a PD-L1 tumor proportion score of 1% to 49% who received chemoimmunotherapy (n = 504) or chemotherapy (n = 347) between March 2017 and June 2022. After adjustment by propensity score matching, the median overall survival (OS) was 22.3 months in the chemoimmunotherapy group and 17.0 months in the chemotherapy-alone group (P = 0.01). Multivariate analysis showed that among 12 clinical factors, liver metastases (P = 0.001) and history of antibiotic use (P = 0.02) were independently associated with shorter OS in the chemoimmunotherapy group. Patients with liver metastases (OS, P = 0.4; progression-free survival, P = 0.06) or history of antimicrobial use (OS, P = 0.24; progression-free survival, P = 0.09) did not benefit from the addition of ICI to chemotherapy. Patients with a history of antimicrobial use experienced more severe pneumonitis with chemoimmunotherapy than all patients (P = 0.04). This cohort study showed that liver metastases and prior antimicrobial therapy are the most important clinical factors that attenuate the efficacy of chemoimmunotherapy in patients with low PD-L1 expression.
Significance: This study shows that liver metastases and prior antibiotic use are key factors for chemoimmunotherapy in advanced NSCLC cases with low PD-L1 expression. They reduce the benefit of adding ICIs to chemotherapy, underscoring the need for new strategies to improve ICI efficacy in patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


