{"title":"吸入左氧氟沙星与粘菌素联合美罗培南治疗多重耐药革兰氏阴性菌所致呼吸机相关性肺炎的疗效比较:一项随机开放标签临床试验","authors":"Masoumeh Sohrabi, Shahram Ala, Afshin Gholipour-Baradari, Fatemeh Heydari, Alireza Nikzad Jamnani, Mahmoud Mousazadeh, Hamidreza Namvar","doi":"10.4103/jrpp.jrpp_12_25","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Ventilator-associated pneumonia (VAP) caused by multidrug-resistant Gram-negative bacteria (MDR-GNB) is a major intensive care unit challenge, particularly in Iran, due to limited antibiotic options. This study compared the efficacy of adding levofloxacin and colistin inhalation form to the baseline regimen of colistin and meropenem in treating VAP caused by MDR-GNB.</p><p><strong>Methods: </strong>Patients with VAP were randomly assigned to the colistin group (<i>n</i> = 24), receiving 2 million international unit (MIU) every 8 h, and the levofloxacin group (<i>n</i> = 22), receiving 250 mg every 12 h, alongside intravenous colistin (4.5 MIU every 12 h) and meropenem (1 g every 8 h). Clinical improvement using the Clinical Pulmonary Infection Score (CPIS) on days 1, 5, and 7, the clinical response on day 7, and inflammatory markers (erythrocyte sedimentation rate and C-reactive protein) on days 1, 3, 5, and 7 were evaluated.</p><p><strong>Findings: </strong>CPIS scores significantly decreased in both groups: Colistin (-3.67 ± 2.14, <i>P</i> < 0.001) and levofloxacin (-4.41 ± 1.71, <i>P</i> < 0.001), with no intergroup difference (<i>P</i> = 0.200). The clinical response analysis indicated that levofloxacin was associated with fewer treatment failures and more partial responses, whereas colistin demonstrated higher rates of complete response; however, these differences were not statistically significant (<i>P</i> > 0.05). Acute kidney injury occurred only in the colistin group (<i>n</i> = 8; 33.3%). Bronchospasm and cough occurred in one levofloxacin patient (4.54%), showing a significant difference in adverse effects (<i>P</i> = 0.004). Mortality rates were higher in the colistin group (<i>n</i> = 17; 70.8%) compared to the levofloxacin group (<i>n</i> = 10; 45.5%), though this difference was not statistically significant (<i>P</i> = 0.08).</p><p><strong>Conclusion: </strong>Levofloxacin inhalation may be considered an effective alternative to colistin inhalation for treating VAP caused by MDR-GNB. It offers similar efficacy and lower nephrotoxicity.</p>","PeriodicalId":17158,"journal":{"name":"Journal of Research in Pharmacy Practice","volume":"14 1","pages":"9-17"},"PeriodicalIF":0.7000,"publicationDate":"2025-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237181/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of the Efficacy of Adding Inhaled Levofloxacin and Colistin to a Basic Regimen of Colistin and Meropenem in the Treatment of Ventilator-associated Pneumonia Caused by Multidrug-resistant Gram-negative Bacteria: A Randomized Open-label Clinical Trial.\",\"authors\":\"Masoumeh Sohrabi, Shahram Ala, Afshin Gholipour-Baradari, Fatemeh Heydari, Alireza Nikzad Jamnani, Mahmoud Mousazadeh, Hamidreza Namvar\",\"doi\":\"10.4103/jrpp.jrpp_12_25\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Ventilator-associated pneumonia (VAP) caused by multidrug-resistant Gram-negative bacteria (MDR-GNB) is a major intensive care unit challenge, particularly in Iran, due to limited antibiotic options. This study compared the efficacy of adding levofloxacin and colistin inhalation form to the baseline regimen of colistin and meropenem in treating VAP caused by MDR-GNB.</p><p><strong>Methods: </strong>Patients with VAP were randomly assigned to the colistin group (<i>n</i> = 24), receiving 2 million international unit (MIU) every 8 h, and the levofloxacin group (<i>n</i> = 22), receiving 250 mg every 12 h, alongside intravenous colistin (4.5 MIU every 12 h) and meropenem (1 g every 8 h). Clinical improvement using the Clinical Pulmonary Infection Score (CPIS) on days 1, 5, and 7, the clinical response on day 7, and inflammatory markers (erythrocyte sedimentation rate and C-reactive protein) on days 1, 3, 5, and 7 were evaluated.</p><p><strong>Findings: </strong>CPIS scores significantly decreased in both groups: Colistin (-3.67 ± 2.14, <i>P</i> < 0.001) and levofloxacin (-4.41 ± 1.71, <i>P</i> < 0.001), with no intergroup difference (<i>P</i> = 0.200). The clinical response analysis indicated that levofloxacin was associated with fewer treatment failures and more partial responses, whereas colistin demonstrated higher rates of complete response; however, these differences were not statistically significant (<i>P</i> > 0.05). Acute kidney injury occurred only in the colistin group (<i>n</i> = 8; 33.3%). Bronchospasm and cough occurred in one levofloxacin patient (4.54%), showing a significant difference in adverse effects (<i>P</i> = 0.004). Mortality rates were higher in the colistin group (<i>n</i> = 17; 70.8%) compared to the levofloxacin group (<i>n</i> = 10; 45.5%), though this difference was not statistically significant (<i>P</i> = 0.08).</p><p><strong>Conclusion: </strong>Levofloxacin inhalation may be considered an effective alternative to colistin inhalation for treating VAP caused by MDR-GNB. It offers similar efficacy and lower nephrotoxicity.</p>\",\"PeriodicalId\":17158,\"journal\":{\"name\":\"Journal of Research in Pharmacy Practice\",\"volume\":\"14 1\",\"pages\":\"9-17\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-06-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12237181/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Research in Pharmacy Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jrpp.jrpp_12_25\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Research in Pharmacy Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jrpp.jrpp_12_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Comparison of the Efficacy of Adding Inhaled Levofloxacin and Colistin to a Basic Regimen of Colistin and Meropenem in the Treatment of Ventilator-associated Pneumonia Caused by Multidrug-resistant Gram-negative Bacteria: A Randomized Open-label Clinical Trial.
Objective: Ventilator-associated pneumonia (VAP) caused by multidrug-resistant Gram-negative bacteria (MDR-GNB) is a major intensive care unit challenge, particularly in Iran, due to limited antibiotic options. This study compared the efficacy of adding levofloxacin and colistin inhalation form to the baseline regimen of colistin and meropenem in treating VAP caused by MDR-GNB.
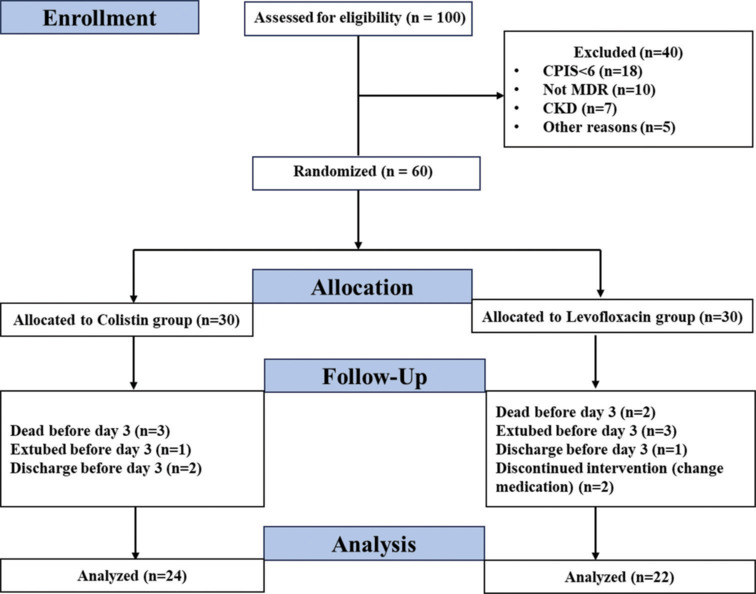
Methods: Patients with VAP were randomly assigned to the colistin group (n = 24), receiving 2 million international unit (MIU) every 8 h, and the levofloxacin group (n = 22), receiving 250 mg every 12 h, alongside intravenous colistin (4.5 MIU every 12 h) and meropenem (1 g every 8 h). Clinical improvement using the Clinical Pulmonary Infection Score (CPIS) on days 1, 5, and 7, the clinical response on day 7, and inflammatory markers (erythrocyte sedimentation rate and C-reactive protein) on days 1, 3, 5, and 7 were evaluated.
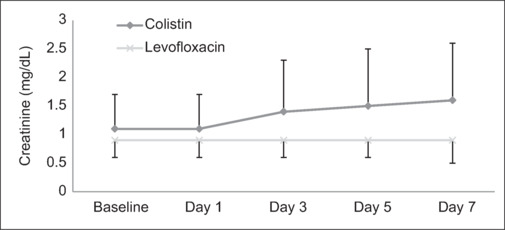
Findings: CPIS scores significantly decreased in both groups: Colistin (-3.67 ± 2.14, P < 0.001) and levofloxacin (-4.41 ± 1.71, P < 0.001), with no intergroup difference (P = 0.200). The clinical response analysis indicated that levofloxacin was associated with fewer treatment failures and more partial responses, whereas colistin demonstrated higher rates of complete response; however, these differences were not statistically significant (P > 0.05). Acute kidney injury occurred only in the colistin group (n = 8; 33.3%). Bronchospasm and cough occurred in one levofloxacin patient (4.54%), showing a significant difference in adverse effects (P = 0.004). Mortality rates were higher in the colistin group (n = 17; 70.8%) compared to the levofloxacin group (n = 10; 45.5%), though this difference was not statistically significant (P = 0.08).
Conclusion: Levofloxacin inhalation may be considered an effective alternative to colistin inhalation for treating VAP caused by MDR-GNB. It offers similar efficacy and lower nephrotoxicity.
期刊介绍:
The main focus of the journal will be on evidence-based drug-related medical researches (with clinical pharmacists’ intervention or documentation), particularly in the Eastern Mediterranean region. However, a wide range of closely related issues will be also covered. These will include clinical studies in the field of pharmaceutical care, reporting adverse drug reactions and human medical toxicology, pharmaco-epidemiology and toxico-epidemiology (poisoning epidemiology), social aspects of pharmacy practice, pharmacy education and economic evaluations of treatment protocols (e.g. cost-effectiveness studies). Local reports of medication utilization studies at hospital or pharmacy levels will only be considered for peer-review process only if they have a new and useful message for the international pharmacy practice professionals and readers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


