Abhishek Maan, Maaz Waseem, Alex Carter, Kirtivardhan Vashishtha, Tarvinder Dhanjal, Jacob Koruth, E Kevin Heist
{"title":"缺血性底物患者室性心动过速的早期与延期导管消融:临床结果的系统回顾和荟萃分析","authors":"Abhishek Maan, Maaz Waseem, Alex Carter, Kirtivardhan Vashishtha, Tarvinder Dhanjal, Jacob Koruth, E Kevin Heist","doi":"10.1093/ehjopen/oeaf076","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Ventricular tachycardia (VT) ablation has been shown to reduce the recurrence of VT episodes, but the timing of performing VT ablation (early; at the time of implantable cardioverter defibrillator implantation) or (deferred: after the patient has received ICD shocks) remains controversial. The objective is to conduct a systematic review and meta-analysis of published data from randomized controlled trials (RCTs) in patients with ischaemic cardiomyopathy (ICM) with the aim of comparing outcome of VT ablation stratified by procedural timing.</p><p><strong>Methods and results: </strong>We conducted a meta-analysis of seven landmark RCTs which included patients with ICM who were either at a high risk of VT or experienced VT/ICD shocks. The primary outcome of VT recurrence was compared according to the timing of performing VT ablation (early vs. deferred). In addition, we also compared the secondary outcome of cardiac mortality. Following a comprehensive search strategy, a total of seven RCTs were included within the final analysis. Based on a pooled analysis, early VT ablation was associated with a significant reduction in the primary outcome [pooled odds ratio (OR) of 0.72, 95% confidence interval (CI): 0.55-0.95, <i>P</i> < 0.05] in comparison with a 'deferred VT ablation' strategy. The cumulative absolute risk reduction (ARR) for the primary outcome was 0.21, and number needed to treat (NNT) to prevent the outcome of VT recurrence was 4.81. Furthermore, the effect size of early VT ablation compared to a deferred VT ablation approach was more pronounced in reduction of ICD shocks in the subgroup of patients with LVEF > 30% vs. those with LVEF < 30% (pooled OR of 0.65, 95% CI of 0.54-0.79, <i>P</i> = 0.01). For the secondary outcomes, we observed that an earlier timing of VT ablation was also associated with both a decrease in cardiac mortality (pooled OR of 0.59, 95% CI of 0.43-0.82) and in the subsequent risk of VT storm (pooled OR of 0.63, 95% CI of 0.51-0.78) when compared with a deferred timing. The cumulative ARR for cardiac mortality was 0.07 and NNT was 15.</p><p><strong>Conclusion: </strong>The findings from this pooled analysis of seven major RCTs suggest that performing early VT ablation may be beneficial in reducing recurrent VT, ICD shocks, and electrical storm and could also improve cardiac mortality. The benefit of performing early VT ablation was greater in patients with LVEF of >30% amongst this ICM cohort.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 4","pages":"oeaf076"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12236160/pdf/","citationCount":"0","resultStr":"{\"title\":\"Early vs. deferred catheter ablation of ventricular tachycardia in patients of ischaemic substrate: systematic review and meta-analysis of clinical outcomes.\",\"authors\":\"Abhishek Maan, Maaz Waseem, Alex Carter, Kirtivardhan Vashishtha, Tarvinder Dhanjal, Jacob Koruth, E Kevin Heist\",\"doi\":\"10.1093/ehjopen/oeaf076\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Ventricular tachycardia (VT) ablation has been shown to reduce the recurrence of VT episodes, but the timing of performing VT ablation (early; at the time of implantable cardioverter defibrillator implantation) or (deferred: after the patient has received ICD shocks) remains controversial. The objective is to conduct a systematic review and meta-analysis of published data from randomized controlled trials (RCTs) in patients with ischaemic cardiomyopathy (ICM) with the aim of comparing outcome of VT ablation stratified by procedural timing.</p><p><strong>Methods and results: </strong>We conducted a meta-analysis of seven landmark RCTs which included patients with ICM who were either at a high risk of VT or experienced VT/ICD shocks. The primary outcome of VT recurrence was compared according to the timing of performing VT ablation (early vs. deferred). In addition, we also compared the secondary outcome of cardiac mortality. Following a comprehensive search strategy, a total of seven RCTs were included within the final analysis. Based on a pooled analysis, early VT ablation was associated with a significant reduction in the primary outcome [pooled odds ratio (OR) of 0.72, 95% confidence interval (CI): 0.55-0.95, <i>P</i> < 0.05] in comparison with a 'deferred VT ablation' strategy. The cumulative absolute risk reduction (ARR) for the primary outcome was 0.21, and number needed to treat (NNT) to prevent the outcome of VT recurrence was 4.81. Furthermore, the effect size of early VT ablation compared to a deferred VT ablation approach was more pronounced in reduction of ICD shocks in the subgroup of patients with LVEF > 30% vs. those with LVEF < 30% (pooled OR of 0.65, 95% CI of 0.54-0.79, <i>P</i> = 0.01). For the secondary outcomes, we observed that an earlier timing of VT ablation was also associated with both a decrease in cardiac mortality (pooled OR of 0.59, 95% CI of 0.43-0.82) and in the subsequent risk of VT storm (pooled OR of 0.63, 95% CI of 0.51-0.78) when compared with a deferred timing. The cumulative ARR for cardiac mortality was 0.07 and NNT was 15.</p><p><strong>Conclusion: </strong>The findings from this pooled analysis of seven major RCTs suggest that performing early VT ablation may be beneficial in reducing recurrent VT, ICD shocks, and electrical storm and could also improve cardiac mortality. The benefit of performing early VT ablation was greater in patients with LVEF of >30% amongst this ICM cohort.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 4\",\"pages\":\"oeaf076\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12236160/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf076\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Early vs. deferred catheter ablation of ventricular tachycardia in patients of ischaemic substrate: systematic review and meta-analysis of clinical outcomes.
Aims: Ventricular tachycardia (VT) ablation has been shown to reduce the recurrence of VT episodes, but the timing of performing VT ablation (early; at the time of implantable cardioverter defibrillator implantation) or (deferred: after the patient has received ICD shocks) remains controversial. The objective is to conduct a systematic review and meta-analysis of published data from randomized controlled trials (RCTs) in patients with ischaemic cardiomyopathy (ICM) with the aim of comparing outcome of VT ablation stratified by procedural timing.
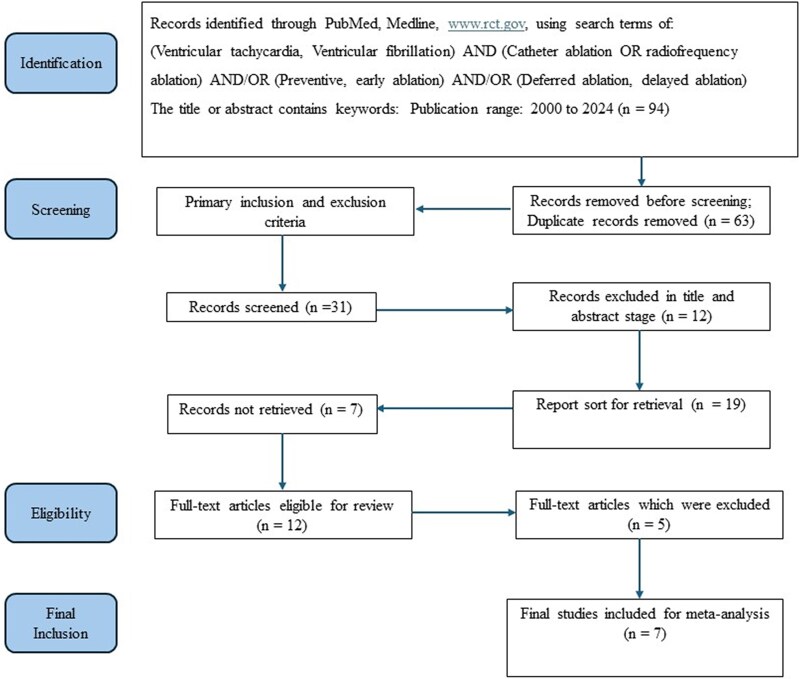
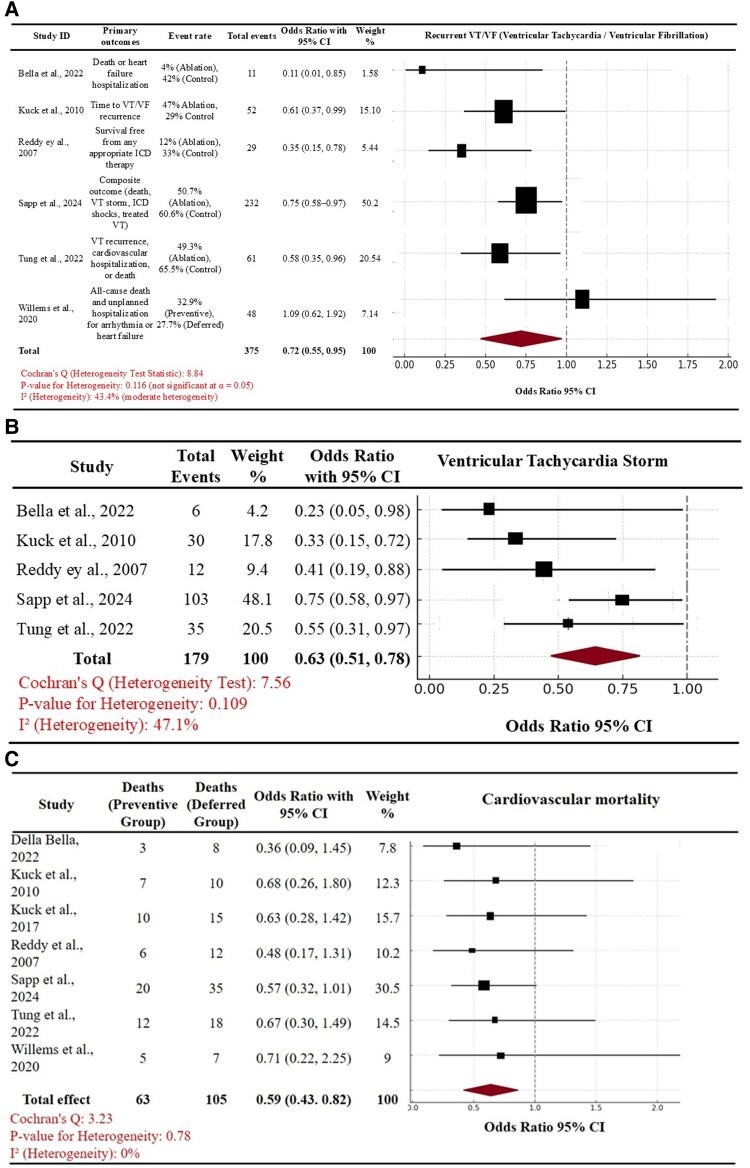
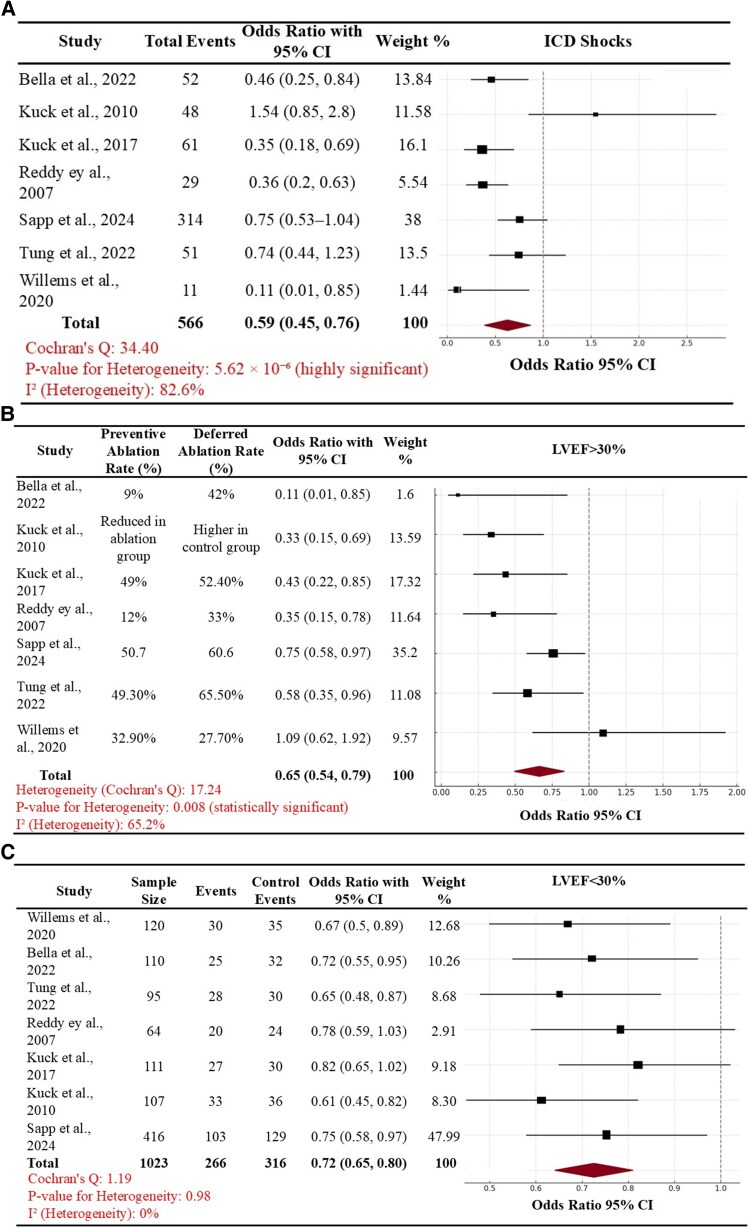
Methods and results: We conducted a meta-analysis of seven landmark RCTs which included patients with ICM who were either at a high risk of VT or experienced VT/ICD shocks. The primary outcome of VT recurrence was compared according to the timing of performing VT ablation (early vs. deferred). In addition, we also compared the secondary outcome of cardiac mortality. Following a comprehensive search strategy, a total of seven RCTs were included within the final analysis. Based on a pooled analysis, early VT ablation was associated with a significant reduction in the primary outcome [pooled odds ratio (OR) of 0.72, 95% confidence interval (CI): 0.55-0.95, P < 0.05] in comparison with a 'deferred VT ablation' strategy. The cumulative absolute risk reduction (ARR) for the primary outcome was 0.21, and number needed to treat (NNT) to prevent the outcome of VT recurrence was 4.81. Furthermore, the effect size of early VT ablation compared to a deferred VT ablation approach was more pronounced in reduction of ICD shocks in the subgroup of patients with LVEF > 30% vs. those with LVEF < 30% (pooled OR of 0.65, 95% CI of 0.54-0.79, P = 0.01). For the secondary outcomes, we observed that an earlier timing of VT ablation was also associated with both a decrease in cardiac mortality (pooled OR of 0.59, 95% CI of 0.43-0.82) and in the subsequent risk of VT storm (pooled OR of 0.63, 95% CI of 0.51-0.78) when compared with a deferred timing. The cumulative ARR for cardiac mortality was 0.07 and NNT was 15.
Conclusion: The findings from this pooled analysis of seven major RCTs suggest that performing early VT ablation may be beneficial in reducing recurrent VT, ICD shocks, and electrical storm and could also improve cardiac mortality. The benefit of performing early VT ablation was greater in patients with LVEF of >30% amongst this ICM cohort.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


