Hugo Barret, Luzia A Niggli, George S Athwal, Robert U Hartzler, Joaquin Sanchez-Sotelo, Floor M Lambers
{"title":"线性和基于区域的方法都提供了准确可靠的测量前肩不稳定相关的盂骨丢失。","authors":"Hugo Barret, Luzia A Niggli, George S Athwal, Robert U Hartzler, Joaquin Sanchez-Sotelo, Floor M Lambers","doi":"10.2106/JBJS.OA.25.00022","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Recurrent anterior shoulder instability may lead to capsuloligamentous and bony lesions of the glenoid and humerus. To date, there is no clear consensus on how to best measure anterior glenoid bone loss (GBL) in the setting of recurrent instability. The objective of this study, therefore, was to evaluate the accuracy and reliability of 7 different methods of measuring anterior GBL on three-dimensional models based on computed tomography.</p><p><strong>Methods: </strong>Eight levels of GBL in the anterior and anteroinferior directions were virtually generated in 14 three-dimensional healthy glenoid models. GBL was measured with 7 different methods: based on a height/width ratio (M1), based on surface area within a circle (M2 and M3), based on linear distance within a circle, (M4, M5, and M6), and based on a volume ratio (M7). For each method, the measurement accuracy was assessed by comparing the calculated value with the true amount of generated GBL. The measurement reliability was assessed by computing the score variance and intraclass correlation coefficient.</p><p><strong>Results: </strong>The most accurate (average measurement error of <2% and largest proportion with error <5%) and reliable (ICC >0.96) measurement methods for GBL were M2 (based on surface area) and M5 (based on the linear distance). The average measurement error for the other methods ranged between 3% and 11% for anterior GBL and between 2% and 9% for anteroinferior GBL. For anterior GBL, the measurement increased by an average of 0.5% for each 1% increase in circle radius, leading to an overestimation of GBL with a larger circle diameter.</p><p><strong>Conclusion: </strong>The methods for calculating glenoid bone loss performed better for the more common direct anterior bone loss rather than the less common anteroinferior-directed bone loss. Both an area-based method (M2) and linear distance-based method (M5) resulted in accurate and reliable measurements of glenoid bone loss; however, the linear distance-based methods may be easier to perform clinically. The height-width ratio and volume methods were less accurate and reliable.</p><p><strong>Level of evidence: </strong>Level IV; case series; diagnostic studies. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 3","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-07-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12225998/pdf/","citationCount":"0","resultStr":"{\"title\":\"Both Linear and Area-based Methods Provide an Accurate and Reliable Measurement of Anterior Shoulder Instability Related Glenoid Bone Loss.\",\"authors\":\"Hugo Barret, Luzia A Niggli, George S Athwal, Robert U Hartzler, Joaquin Sanchez-Sotelo, Floor M Lambers\",\"doi\":\"10.2106/JBJS.OA.25.00022\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Recurrent anterior shoulder instability may lead to capsuloligamentous and bony lesions of the glenoid and humerus. To date, there is no clear consensus on how to best measure anterior glenoid bone loss (GBL) in the setting of recurrent instability. The objective of this study, therefore, was to evaluate the accuracy and reliability of 7 different methods of measuring anterior GBL on three-dimensional models based on computed tomography.</p><p><strong>Methods: </strong>Eight levels of GBL in the anterior and anteroinferior directions were virtually generated in 14 three-dimensional healthy glenoid models. GBL was measured with 7 different methods: based on a height/width ratio (M1), based on surface area within a circle (M2 and M3), based on linear distance within a circle, (M4, M5, and M6), and based on a volume ratio (M7). For each method, the measurement accuracy was assessed by comparing the calculated value with the true amount of generated GBL. The measurement reliability was assessed by computing the score variance and intraclass correlation coefficient.</p><p><strong>Results: </strong>The most accurate (average measurement error of <2% and largest proportion with error <5%) and reliable (ICC >0.96) measurement methods for GBL were M2 (based on surface area) and M5 (based on the linear distance). The average measurement error for the other methods ranged between 3% and 11% for anterior GBL and between 2% and 9% for anteroinferior GBL. For anterior GBL, the measurement increased by an average of 0.5% for each 1% increase in circle radius, leading to an overestimation of GBL with a larger circle diameter.</p><p><strong>Conclusion: </strong>The methods for calculating glenoid bone loss performed better for the more common direct anterior bone loss rather than the less common anteroinferior-directed bone loss. Both an area-based method (M2) and linear distance-based method (M5) resulted in accurate and reliable measurements of glenoid bone loss; however, the linear distance-based methods may be easier to perform clinically. The height-width ratio and volume methods were less accurate and reliable.</p><p><strong>Level of evidence: </strong>Level IV; case series; diagnostic studies. See Instructions for Authors for a complete description of levels of evidence.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"10 3\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-07-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12225998/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.25.00022\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.25.00022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Both Linear and Area-based Methods Provide an Accurate and Reliable Measurement of Anterior Shoulder Instability Related Glenoid Bone Loss.
Background: Recurrent anterior shoulder instability may lead to capsuloligamentous and bony lesions of the glenoid and humerus. To date, there is no clear consensus on how to best measure anterior glenoid bone loss (GBL) in the setting of recurrent instability. The objective of this study, therefore, was to evaluate the accuracy and reliability of 7 different methods of measuring anterior GBL on three-dimensional models based on computed tomography.
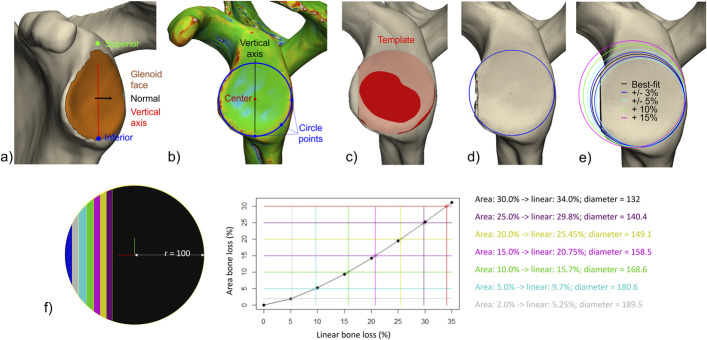
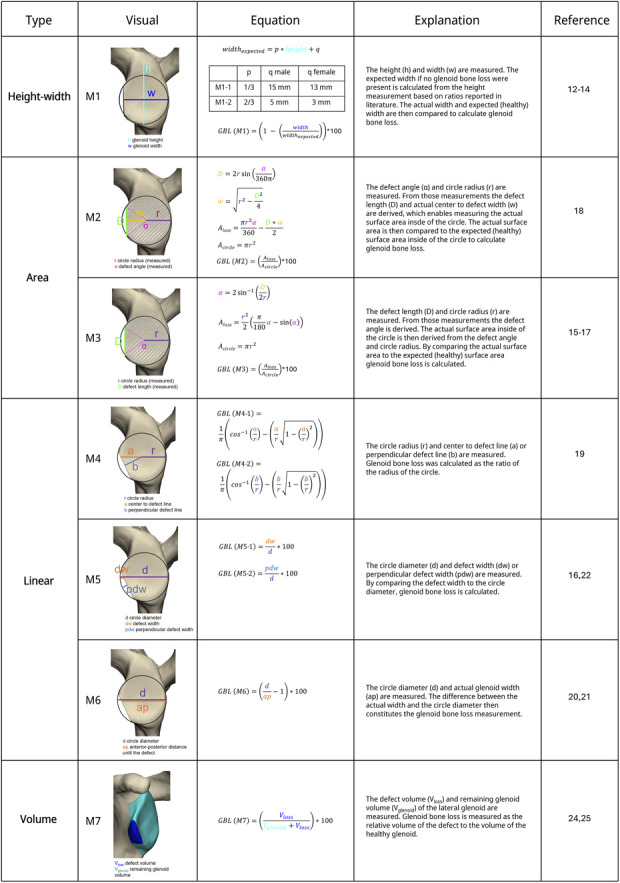
Methods: Eight levels of GBL in the anterior and anteroinferior directions were virtually generated in 14 three-dimensional healthy glenoid models. GBL was measured with 7 different methods: based on a height/width ratio (M1), based on surface area within a circle (M2 and M3), based on linear distance within a circle, (M4, M5, and M6), and based on a volume ratio (M7). For each method, the measurement accuracy was assessed by comparing the calculated value with the true amount of generated GBL. The measurement reliability was assessed by computing the score variance and intraclass correlation coefficient.
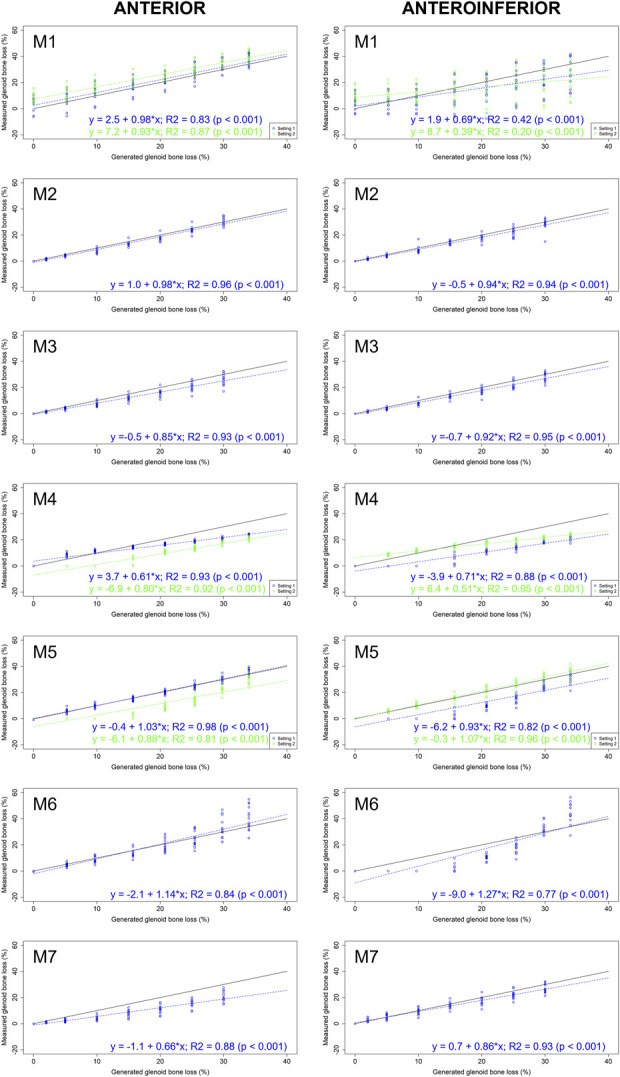
Results: The most accurate (average measurement error of <2% and largest proportion with error <5%) and reliable (ICC >0.96) measurement methods for GBL were M2 (based on surface area) and M5 (based on the linear distance). The average measurement error for the other methods ranged between 3% and 11% for anterior GBL and between 2% and 9% for anteroinferior GBL. For anterior GBL, the measurement increased by an average of 0.5% for each 1% increase in circle radius, leading to an overestimation of GBL with a larger circle diameter.
Conclusion: The methods for calculating glenoid bone loss performed better for the more common direct anterior bone loss rather than the less common anteroinferior-directed bone loss. Both an area-based method (M2) and linear distance-based method (M5) resulted in accurate and reliable measurements of glenoid bone loss; however, the linear distance-based methods may be easier to perform clinically. The height-width ratio and volume methods were less accurate and reliable.
Level of evidence: Level IV; case series; diagnostic studies. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


