David Fritz, Ben Ose, Hannah Zerr, Maci Clark, Caroline Trupp, Amulya Gupta, Ahmed Shahab, Seth H Sheldon, Amit Noheria
{"title":"从传统的右心室起搏到左束分支区域起搏的影响。","authors":"David Fritz, Ben Ose, Hannah Zerr, Maci Clark, Caroline Trupp, Amulya Gupta, Ahmed Shahab, Seth H Sheldon, Amit Noheria","doi":"10.19102/icrm.2025.16064","DOIUrl":null,"url":null,"abstract":"<p><p>Left bundle branch area pacing (LBBAP) may mitigate pacing-induced cardiomyopathy (PICM) and is increasingly favored over traditional right ventricular pacing (RVP). We sought to evaluate the impact of a practice-wide switch from RVP to LBBAP. We switched practice from RVP to primarily LBBAP at our center in 2020. A retrospective review was conducted to compare patients who underwent LBBAP from 2020-2023 with controls who underwent RVP from 2018-2019. The LBBAP (n = 288; age, 73.3 ± 10.7 years; left ventricular ejection fraction [LVEF], 56.9% ± 11.4%) and RVP (n = 172) groups were similar in terms of age, body mass index, hypertension, diabetes, and LVEF. The LBBAP group as compared to the RVP group had fewer women (38% vs. 51%; <i>P</i> = .006) and longer intrinsic conducted QRS durations (117 ± 28 vs. 110 ± 30 ms; <i>P</i> = .04). LBBAP devices required longer implant (102 vs. 67 min) and fluoroscopy (9.3 vs. 6.9 min) times but resulted in shorter paced QRS durations (122 ± 20 vs. 145 ± 24 ms; all <i>P</i> < .0001). At 3 months, LBBAP patients had higher sensing (13.8 ± 6.1 vs. 12.0 ± 5.6 mV; <i>P</i> = .007), lower pacing impedance (543 ± 98 vs. 576 ± 150 Ω; <i>P</i> = .008), and similar capture threshold (0.78 ± 0.24 vs. 0.76 ± 0.35 V; <i>P</i> = .5) values. Device-related adverse events were similar between the groups (LBBAP 8.7% vs. RVP 8.8%; <i>P</i> = 1.0), which included ventricular lead dislodgement (2.1% vs. 0.6%; <i>P</i> = .3). There were no differences in hazard rates of all-cause mortality (<i>P</i> = .5) or heart failure (HF) hospitalizations (<i>P</i> = .07). In a subgroup of patients with ≥20% ventricular pacing, the average LVEF change during follow-up in the LBBAP group as opposed to the RVP group was +1.6% ± 12.9% versus -3.8% ± 12.0% (<i>P</i> = .03), the average left ventricular internal diameter at end-diastole change was -0.18 ± 0.73 cm versus +0.16 ± 0.45 cm (<i>P</i> = .006), and there were no differences in the hazard rate of all-cause mortality (<i>P</i> = .6) or HF hospitalizations (<i>P</i> = 1.0). Our results suggest there were no adverse consequences of the practice-wide switch from RVP to LBBAP. LBBAP was associated with longer procedure and fluoroscopy times but resulted in narrower paced QRS durations and less PICM.</p>","PeriodicalId":36299,"journal":{"name":"Journal of Innovations in Cardiac Rhythm Management","volume":"16 6","pages":"6297-6305"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12233320/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of a Practice-wide Switch from Traditional Right Ventricular Pacing to Left Bundle Branch Area Pacing.\",\"authors\":\"David Fritz, Ben Ose, Hannah Zerr, Maci Clark, Caroline Trupp, Amulya Gupta, Ahmed Shahab, Seth H Sheldon, Amit Noheria\",\"doi\":\"10.19102/icrm.2025.16064\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Left bundle branch area pacing (LBBAP) may mitigate pacing-induced cardiomyopathy (PICM) and is increasingly favored over traditional right ventricular pacing (RVP). We sought to evaluate the impact of a practice-wide switch from RVP to LBBAP. We switched practice from RVP to primarily LBBAP at our center in 2020. A retrospective review was conducted to compare patients who underwent LBBAP from 2020-2023 with controls who underwent RVP from 2018-2019. The LBBAP (n = 288; age, 73.3 ± 10.7 years; left ventricular ejection fraction [LVEF], 56.9% ± 11.4%) and RVP (n = 172) groups were similar in terms of age, body mass index, hypertension, diabetes, and LVEF. The LBBAP group as compared to the RVP group had fewer women (38% vs. 51%; <i>P</i> = .006) and longer intrinsic conducted QRS durations (117 ± 28 vs. 110 ± 30 ms; <i>P</i> = .04). LBBAP devices required longer implant (102 vs. 67 min) and fluoroscopy (9.3 vs. 6.9 min) times but resulted in shorter paced QRS durations (122 ± 20 vs. 145 ± 24 ms; all <i>P</i> < .0001). At 3 months, LBBAP patients had higher sensing (13.8 ± 6.1 vs. 12.0 ± 5.6 mV; <i>P</i> = .007), lower pacing impedance (543 ± 98 vs. 576 ± 150 Ω; <i>P</i> = .008), and similar capture threshold (0.78 ± 0.24 vs. 0.76 ± 0.35 V; <i>P</i> = .5) values. Device-related adverse events were similar between the groups (LBBAP 8.7% vs. RVP 8.8%; <i>P</i> = 1.0), which included ventricular lead dislodgement (2.1% vs. 0.6%; <i>P</i> = .3). There were no differences in hazard rates of all-cause mortality (<i>P</i> = .5) or heart failure (HF) hospitalizations (<i>P</i> = .07). In a subgroup of patients with ≥20% ventricular pacing, the average LVEF change during follow-up in the LBBAP group as opposed to the RVP group was +1.6% ± 12.9% versus -3.8% ± 12.0% (<i>P</i> = .03), the average left ventricular internal diameter at end-diastole change was -0.18 ± 0.73 cm versus +0.16 ± 0.45 cm (<i>P</i> = .006), and there were no differences in the hazard rate of all-cause mortality (<i>P</i> = .6) or HF hospitalizations (<i>P</i> = 1.0). Our results suggest there were no adverse consequences of the practice-wide switch from RVP to LBBAP. LBBAP was associated with longer procedure and fluoroscopy times but resulted in narrower paced QRS durations and less PICM.</p>\",\"PeriodicalId\":36299,\"journal\":{\"name\":\"Journal of Innovations in Cardiac Rhythm Management\",\"volume\":\"16 6\",\"pages\":\"6297-6305\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12233320/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Innovations in Cardiac Rhythm Management\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.19102/icrm.2025.16064\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Innovations in Cardiac Rhythm Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.19102/icrm.2025.16064","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
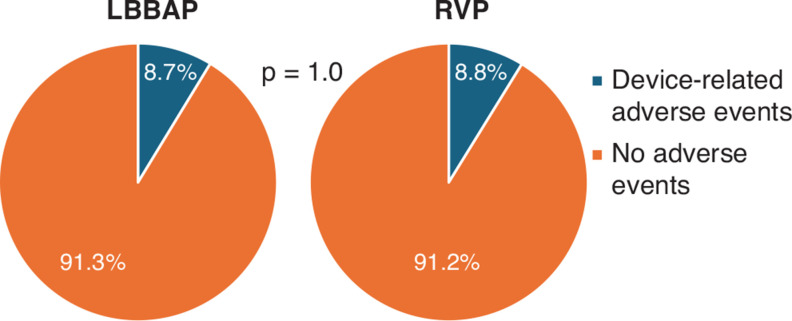
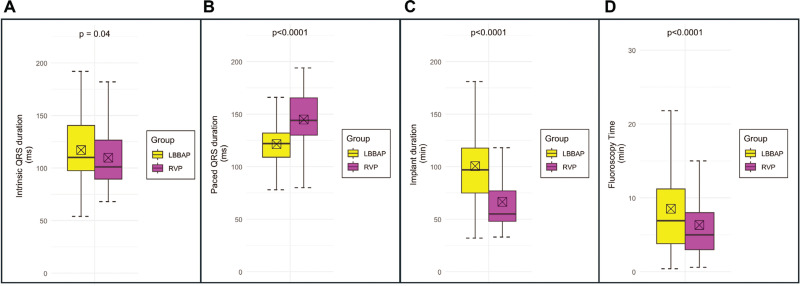
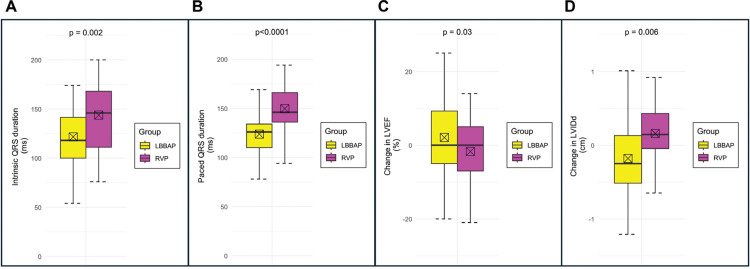
左束分支区起搏(LBBAP)可以减轻起搏诱导的心肌病(PICM),并且越来越受到传统右室起搏(RVP)的青睐。我们试图评估从RVP到LBBAP的实践范围转换的影响。2020年,我们中心的实践从RVP转为以LBBAP为主。一项回顾性研究比较了2020-2023年接受LBBAP的患者和2018-2019年接受RVP的对照组。LBBAP (n = 288;年龄:73.3±10.7岁;左心室射血分数[LVEF], 56.9%±11.4%)和RVP (n = 172)组在年龄、体重指数、高血压、糖尿病和LVEF方面相似。与RVP组相比,LBBAP组的女性人数较少(38% vs. 51%;P = 0.006)和更长的本征传导QRS持续时间(117±28 vs 110±30 ms;P = .04)。LBBAP装置需要更长的植入时间(102 vs. 67分钟)和透视时间(9.3 vs. 6.9分钟),但QRS持续时间较短(122±20 vs. 145±24 ms);P < 0.0001)。在3个月时,LBBAP患者的感觉更高(13.8±6.1 vs 12.0±5.6 mV;P = .007),较低的起搏阻抗(543±98 vs. 576±150 Ω;P = 0.008),相似的捕获阈值(0.78±0.24 vs. 0.76±0.35 V;P = .5)值。两组之间器械相关不良事件相似(LBBAP 8.7% vs RVP 8.8%;P = 1.0),包括心室导联脱位(2.1% vs. 0.6%;P = .3)。两组全因死亡率(P = 0.5)和心力衰竭住院率(P = 0.07)无差异。子组的患者心室≥20%,平均LVEF改变LBBAP组在随访中而不是RVP组+ 1.6%±12.9%和-3.8%±12.0% (P = . 03),左心室内部直径平均end-diastole变化是-0.18±0.73厘米和+ 0.16±0.45厘米(P = .006),和没有差异的故障率(P = 0。6)或心力衰竭住院患者全因死亡率(P = 1.0)。我们的研究结果表明,从RVP到LBBAP的广泛实践转换没有不良后果。LBBAP与较长的手术和透视时间相关,但导致较窄的QRS持续时间和较低的PICM。
Impact of a Practice-wide Switch from Traditional Right Ventricular Pacing to Left Bundle Branch Area Pacing.
Left bundle branch area pacing (LBBAP) may mitigate pacing-induced cardiomyopathy (PICM) and is increasingly favored over traditional right ventricular pacing (RVP). We sought to evaluate the impact of a practice-wide switch from RVP to LBBAP. We switched practice from RVP to primarily LBBAP at our center in 2020. A retrospective review was conducted to compare patients who underwent LBBAP from 2020-2023 with controls who underwent RVP from 2018-2019. The LBBAP (n = 288; age, 73.3 ± 10.7 years; left ventricular ejection fraction [LVEF], 56.9% ± 11.4%) and RVP (n = 172) groups were similar in terms of age, body mass index, hypertension, diabetes, and LVEF. The LBBAP group as compared to the RVP group had fewer women (38% vs. 51%; P = .006) and longer intrinsic conducted QRS durations (117 ± 28 vs. 110 ± 30 ms; P = .04). LBBAP devices required longer implant (102 vs. 67 min) and fluoroscopy (9.3 vs. 6.9 min) times but resulted in shorter paced QRS durations (122 ± 20 vs. 145 ± 24 ms; all P < .0001). At 3 months, LBBAP patients had higher sensing (13.8 ± 6.1 vs. 12.0 ± 5.6 mV; P = .007), lower pacing impedance (543 ± 98 vs. 576 ± 150 Ω; P = .008), and similar capture threshold (0.78 ± 0.24 vs. 0.76 ± 0.35 V; P = .5) values. Device-related adverse events were similar between the groups (LBBAP 8.7% vs. RVP 8.8%; P = 1.0), which included ventricular lead dislodgement (2.1% vs. 0.6%; P = .3). There were no differences in hazard rates of all-cause mortality (P = .5) or heart failure (HF) hospitalizations (P = .07). In a subgroup of patients with ≥20% ventricular pacing, the average LVEF change during follow-up in the LBBAP group as opposed to the RVP group was +1.6% ± 12.9% versus -3.8% ± 12.0% (P = .03), the average left ventricular internal diameter at end-diastole change was -0.18 ± 0.73 cm versus +0.16 ± 0.45 cm (P = .006), and there were no differences in the hazard rate of all-cause mortality (P = .6) or HF hospitalizations (P = 1.0). Our results suggest there were no adverse consequences of the practice-wide switch from RVP to LBBAP. LBBAP was associated with longer procedure and fluoroscopy times but resulted in narrower paced QRS durations and less PICM.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


