Wilmer Santiago Herrera Malpica, Jully C Gómez, Fernando Ortiz-Corredor, Paula Vanessa Muñetones Hernández, Cristian Correa-Arrieta
{"title":"COL6A1基因c.788G > A变异的Bethlem肌病的多模态评估:1例与遗传、超声和结构功能不一致相关的病例报告","authors":"Wilmer Santiago Herrera Malpica, Jully C Gómez, Fernando Ortiz-Corredor, Paula Vanessa Muñetones Hernández, Cristian Correa-Arrieta","doi":"10.36185/2532-1900-1028","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Bethlem myopathy (BM) is a collagen-VI-related myopathy caused by mutations in the COL6A1, COL6A2, and COL6A3 genes. It is characterized by proximal muscle weakness, distal joint laxity, and contractures, with symptoms appearing during childhood and progressing slowly. Muscle ultrasound, using tools like the Heckmatt scale, complements genetic analysis and provides noninvasive insights into muscle pathology, particularly in atypical presentations.</p><p><strong>Case report: </strong>An 8-year-old male presented with muscle weakness since birth, delayed motor milestones, toe walking, and frequent falls. Family history revealed maternal-line neuromuscular disorders. Clinical examination showed hyporeflexia, thoracic hypotrophy, and decreased proximal muscle strength, alongside joint hypermobility and keratosis pilaris. Electromyography indicated a myopathic pattern in proximal upper limb muscles. Genetic analysis confirmed a pathogenic COL6A1 variant (c.788G > A, p.Gly263Asp). Ultrasound findings revealed advanced structural compromise with Heckmatt grade IV echogenicity in the deltoid, iliopsoas, and rectus femoris, indicating fatty infiltration and fibrosis. Functional tests, including Motor Function Measurement (MFM), showed adequate performance despite significant structural abnormalities.</p><p><strong>Discussion: </strong>This case illustrates the diagnostic challenges of BM, characterized by phenotypic variability and the complexity of correlating structural and functional findings. Muscle ultrasound findings demonstrated advanced echogenic changes, but functional performance remained preserved, highlighting a mismatch between structural changes and functional outcomes.</p><p><strong>Conclusion: </strong>This case highlights the diagnostic challenges of BM, where a patient with a COL6A1 gene mutation exhibited significant muscle abnormalities on ultrasound but maintained relatively preserved motor function according to the MFM scale. This discrepancy emphasizes the limitations of functional assessments like MFM in capturing the extent of muscle weakness. Ultrasound and dynamometry provided a more comprehensive evaluation, underscoring the importance of integrating structural and functional assessments for accurate diagnosis and management. This case stresses the need for an individualized approach in managing BM, considering both genetic and clinical findings.</p>","PeriodicalId":93851,"journal":{"name":"Acta myologica : myopathies and cardiomyopathies : official journal of the Mediterranean Society of Myology","volume":"44 2","pages":"57-61"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12250587/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multimodal Evaluation of Bethlem Myopathy with the c.788G > A Variant in the COL6A1 Gene: a case report with genetic, ultrasonographic, and structural-functional discordance correlations.\",\"authors\":\"Wilmer Santiago Herrera Malpica, Jully C Gómez, Fernando Ortiz-Corredor, Paula Vanessa Muñetones Hernández, Cristian Correa-Arrieta\",\"doi\":\"10.36185/2532-1900-1028\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Bethlem myopathy (BM) is a collagen-VI-related myopathy caused by mutations in the COL6A1, COL6A2, and COL6A3 genes. It is characterized by proximal muscle weakness, distal joint laxity, and contractures, with symptoms appearing during childhood and progressing slowly. Muscle ultrasound, using tools like the Heckmatt scale, complements genetic analysis and provides noninvasive insights into muscle pathology, particularly in atypical presentations.</p><p><strong>Case report: </strong>An 8-year-old male presented with muscle weakness since birth, delayed motor milestones, toe walking, and frequent falls. Family history revealed maternal-line neuromuscular disorders. Clinical examination showed hyporeflexia, thoracic hypotrophy, and decreased proximal muscle strength, alongside joint hypermobility and keratosis pilaris. Electromyography indicated a myopathic pattern in proximal upper limb muscles. Genetic analysis confirmed a pathogenic COL6A1 variant (c.788G > A, p.Gly263Asp). Ultrasound findings revealed advanced structural compromise with Heckmatt grade IV echogenicity in the deltoid, iliopsoas, and rectus femoris, indicating fatty infiltration and fibrosis. Functional tests, including Motor Function Measurement (MFM), showed adequate performance despite significant structural abnormalities.</p><p><strong>Discussion: </strong>This case illustrates the diagnostic challenges of BM, characterized by phenotypic variability and the complexity of correlating structural and functional findings. Muscle ultrasound findings demonstrated advanced echogenic changes, but functional performance remained preserved, highlighting a mismatch between structural changes and functional outcomes.</p><p><strong>Conclusion: </strong>This case highlights the diagnostic challenges of BM, where a patient with a COL6A1 gene mutation exhibited significant muscle abnormalities on ultrasound but maintained relatively preserved motor function according to the MFM scale. This discrepancy emphasizes the limitations of functional assessments like MFM in capturing the extent of muscle weakness. Ultrasound and dynamometry provided a more comprehensive evaluation, underscoring the importance of integrating structural and functional assessments for accurate diagnosis and management. This case stresses the need for an individualized approach in managing BM, considering both genetic and clinical findings.</p>\",\"PeriodicalId\":93851,\"journal\":{\"name\":\"Acta myologica : myopathies and cardiomyopathies : official journal of the Mediterranean Society of Myology\",\"volume\":\"44 2\",\"pages\":\"57-61\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12250587/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta myologica : myopathies and cardiomyopathies : official journal of the Mediterranean Society of Myology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36185/2532-1900-1028\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta myologica : myopathies and cardiomyopathies : official journal of the Mediterranean Society of Myology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36185/2532-1900-1028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
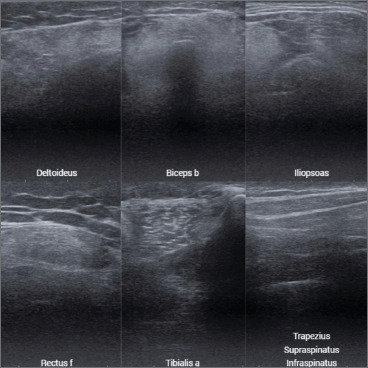
介绍:Bethlem myopathy (BM)是一种由COL6A1、COL6A2和COL6A3基因突变引起的与胶原vi相关的肌病。其特点是近端肌肉无力,远端关节松弛和挛缩,症状出现在儿童时期,进展缓慢。肌肉超声,使用Heckmatt量表等工具,补充了基因分析,并提供了对肌肉病理的非侵入性见解,特别是在非典型表现中。病例报告:一名8岁男性,自出生以来表现为肌肉无力,运动里程碑延迟,脚趾行走,经常跌倒。家族史显示母系神经肌肉疾病。临床检查显示反射减退,胸肌萎缩,近端肌力下降,同时伴有关节活动过度和角化症。肌电图显示上肢近端肌肉呈肌病型。遗传分析证实了COL6A1致病性变异(c.788G > a, p.Gly263Asp)。超声结果显示,三角肌、髂腰肌和股直肌出现了严重的结构损伤,伴有Heckmatt IV级回声,表明脂肪浸润和纤维化。功能测试,包括运动功能测量(MFM),尽管有明显的结构异常,但表现良好。讨论:该病例说明了BM的诊断挑战,其特征是表型变异性和相关结构和功能发现的复杂性。肌肉超声结果显示出严重的回声改变,但功能表现保持不变,突出了结构变化和功能结果之间的不匹配。结论:该病例突出了BM的诊断挑战,COL6A1基因突变的患者在超声上表现出明显的肌肉异常,但根据MFM量表维持相对保留的运动功能。这种差异强调了MFM等功能评估在捕捉肌肉无力程度方面的局限性。超声和动力测量提供了更全面的评估,强调了整合结构和功能评估对准确诊断和管理的重要性。本病例强调在考虑遗传和临床结果的情况下,需要个体化的方法来管理BM。
Multimodal Evaluation of Bethlem Myopathy with the c.788G > A Variant in the COL6A1 Gene: a case report with genetic, ultrasonographic, and structural-functional discordance correlations.
Introduction: Bethlem myopathy (BM) is a collagen-VI-related myopathy caused by mutations in the COL6A1, COL6A2, and COL6A3 genes. It is characterized by proximal muscle weakness, distal joint laxity, and contractures, with symptoms appearing during childhood and progressing slowly. Muscle ultrasound, using tools like the Heckmatt scale, complements genetic analysis and provides noninvasive insights into muscle pathology, particularly in atypical presentations.
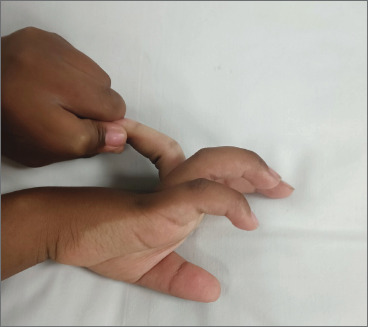
Case report: An 8-year-old male presented with muscle weakness since birth, delayed motor milestones, toe walking, and frequent falls. Family history revealed maternal-line neuromuscular disorders. Clinical examination showed hyporeflexia, thoracic hypotrophy, and decreased proximal muscle strength, alongside joint hypermobility and keratosis pilaris. Electromyography indicated a myopathic pattern in proximal upper limb muscles. Genetic analysis confirmed a pathogenic COL6A1 variant (c.788G > A, p.Gly263Asp). Ultrasound findings revealed advanced structural compromise with Heckmatt grade IV echogenicity in the deltoid, iliopsoas, and rectus femoris, indicating fatty infiltration and fibrosis. Functional tests, including Motor Function Measurement (MFM), showed adequate performance despite significant structural abnormalities.
Discussion: This case illustrates the diagnostic challenges of BM, characterized by phenotypic variability and the complexity of correlating structural and functional findings. Muscle ultrasound findings demonstrated advanced echogenic changes, but functional performance remained preserved, highlighting a mismatch between structural changes and functional outcomes.
Conclusion: This case highlights the diagnostic challenges of BM, where a patient with a COL6A1 gene mutation exhibited significant muscle abnormalities on ultrasound but maintained relatively preserved motor function according to the MFM scale. This discrepancy emphasizes the limitations of functional assessments like MFM in capturing the extent of muscle weakness. Ultrasound and dynamometry provided a more comprehensive evaluation, underscoring the importance of integrating structural and functional assessments for accurate diagnosis and management. This case stresses the need for an individualized approach in managing BM, considering both genetic and clinical findings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


